

A randomized trial of recombinant human granulocyte-macrophage colony stimulating factor for patients with acute lung injury
- PMID: 21926600
- PMCID: PMC3242850
- DOI: 10.1097/CCM.0b013e31822d7bf0
A randomized trial of recombinant human granulocyte-macrophage colony stimulating factor for patients with acute lung injury
Abstract
Rationale: Despite recent advances in critical care and ventilator management, acute lung injury and acute respiratory distress syndrome continue to cause significant morbidity and mortality. Granulocyte-macrophage colony stimulating factor may be beneficial for patients with acute respiratory distress syndrome.
Objectives: To determine whether intravenous infusion of granulocyte-macrophage colony stimulating factor would improve clinical outcomes for patients with acute lung injury/acute respiratory distress syndrome.
Design: A randomized, double-blind, placebo-controlled clinical trial of human recombinant granulocyte-macrophage colony stimulating factor vs. placebo. The primary outcome was days alive and breathing without mechanical ventilatory support within the first 28 days after randomization. Secondary outcomes included mortality and organ failure-free days.
Setting: Medical and surgical intensive care units at three academic medical centers.
Patients: One hundred thirty individuals with acute lung injury of at least 3 days duration were enrolled, out of a planned cohort of 200 subjects.
Interventions: Patients were randomized to receive human recombinant granulocyte-macrophage colony stimulating factor (64 subjects, 250 μg/M) or placebo (66 subjects) by intravenous infusion daily for 14 days. Patients received mechanical ventilation using a lung-protective protocol.
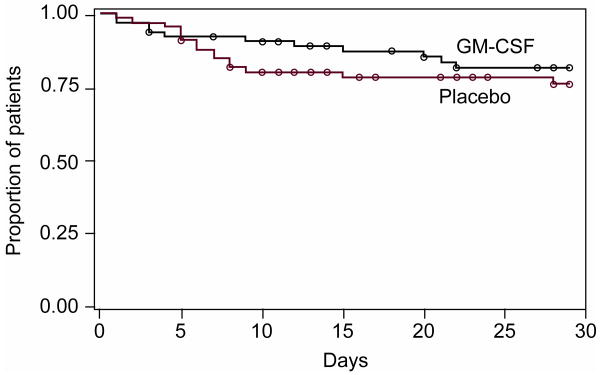
Measurements and main results: There was no difference in ventilator-free days between groups (10.7 ± 10.3 days placebo vs. 10.8 ± 10.5 days granulocyte-macrophage colony stimulating factor, p = .82). Differences in 28-day mortality (23% in placebo vs. 17% in patients receiving granulocyte-macrophage colony stimulating factor (p = .31) and organ failure-free days (12.8 ± 11.3 days placebo vs. 15.7 ± 11.9 days granulocyte-macrophage colony stimulating factor, p = .16) were not statistically significant. There were similar numbers of serious adverse events in each group.
Conclusions: In a randomized phase II trial, granulocyte-macrophage colony stimulating factor treatment did not increase the number of ventilator-free days in patients with acute lung injury/acute respiratory distress syndrome. A larger trial would be required to determine whether treatment with granulocyte-macrophage colony stimulating factor might alter important clinical outcomes, such as mortality or multiorgan failure. (ClinicalTrials.gov number, NCT00201409 [ClinicalTrials.gov]).
Figures
Comment in
-
Another "negative" acute lung injury trial.Crit Care Med. 2012 Jan;40(1):315-6. doi: 10.1097/CCM.0b013e318232d307. Crit Care Med. 2012. PMID: 22179356 No abstract available.
References
-
- Ware LB, Matthay MA. The Acute Respiratory Distress Syndrome. N Engl J Med. 2000;342(18):1334–1349. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and Outcomes of Acute Lung Injury. N Engl J Med. 2005;353(16):1685–1693. - PubMed
-
- Ashbaugh DG, Bigelow DB, Petty TL, et al. Acute respiratory distress in adults. Lancet. 1967;2(7511):319–323. - PubMed
-
- Steinberg KP, Hudson LD. Acute lung injury and acute respiratory distress syndrome. The clinical syndrome. Clinics in Chest Medicine. 2000;21(3):401–417. vii. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N Engl J Med. 2000;342(18):1301–1308. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
