

Review
doi: 10.3348/kjr.2011.12.5.525.
Epub 2011 Aug 24.
Thermal ablation for benign thyroid nodules: radiofrequency and laser
Affiliations
- PMID: 21927553
- PMCID: PMC3168793
- DOI: 10.3348/kjr.2011.12.5.525
Item in Clipboard
Review
Thermal ablation for benign thyroid nodules: radiofrequency and laser
Korean J Radiol.
2011 Sep-Oct.
Abstract
Although ethanol ablation has been successfully used to treat cystic thyroid nodules, this procedure is less effective when the thyroid nodules are solid. Radiofrequency (RF) ablation, a newer procedure used to treat malignant liver tumors, has been valuable in the treatment of benign thyroid nodules regardless of the extent of the solid component. This article reviews the basic physics, techniques, applications, results, and complications of thyroid RF ablation, in comparison to laser ablation.
Keywords: Ethanol ablation; Laser ablation; Radiofrequency ablation; Thyroid nodule; Ultrasonography.
Figures
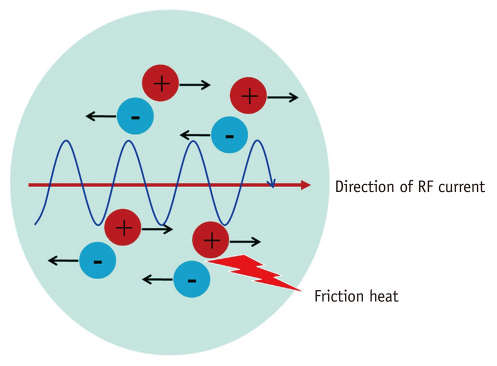
Ionic agitation and formation of frictional heat. Tissue ions are agitated by application of alternating electric current. Ionic agitation results in ion friction, which in turn causes heat production. RF = radiofrequency.
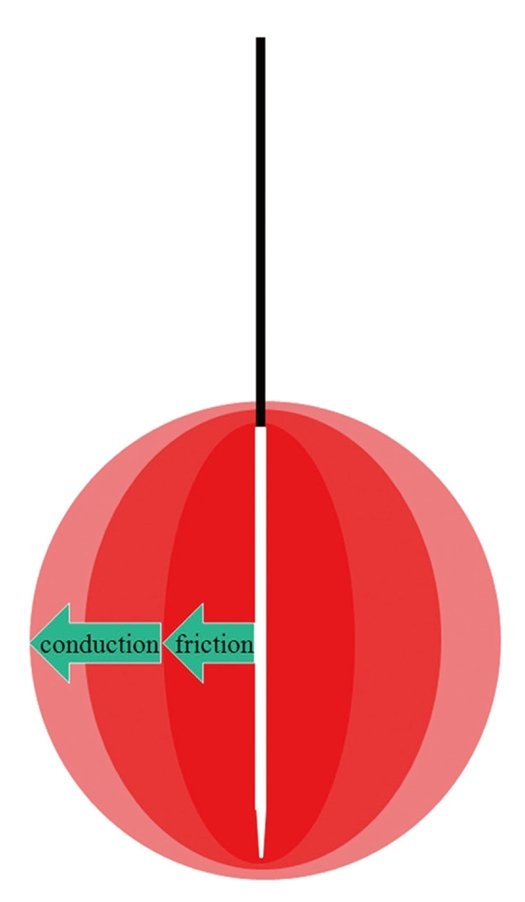
Heat propagation through target tumor. Immediate tissue coagulation necrosis is achieved by frictional heat generated in vicinity of electrode, but electrode-remote tumor tissue is ablated more slowly, via conductive heat.
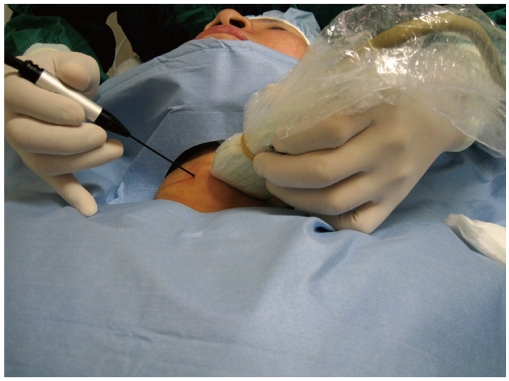
Positions of operator and patient. Patient is placed in supine position with mild neck extension, and operator stands close to patient's head. Left hand of operator holds US probe and right hand of electrode.
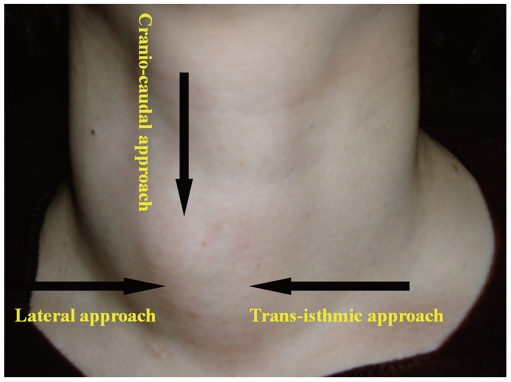
Three-method approach method employing electrode. Trans-isthmic approach via short axis of thyroid nodule (from medial to lateral aspect) is used in Korea. When vessels appear to be prominent on trans-isthmic approach route, lateral approach may prevent vessel injury. Cranio-caudal (longitudinal) approach, through axis of thyroid nodule, has been used in Italy for both radiofrequency ablation and percutaneous laser ablation.
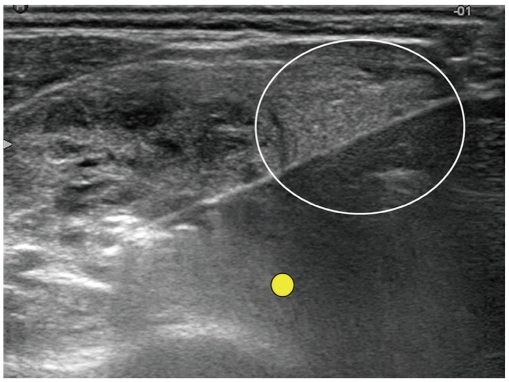
US image showing trans-isthmic approach. This transverse US image shows electrode in its entirety, thyroid nodule, and possible location of recurrent laryngeal nerve (small yellow circle). Electrode passes through volume of thyroid parenchyma (white circle) adequate to prevent electrode movement.
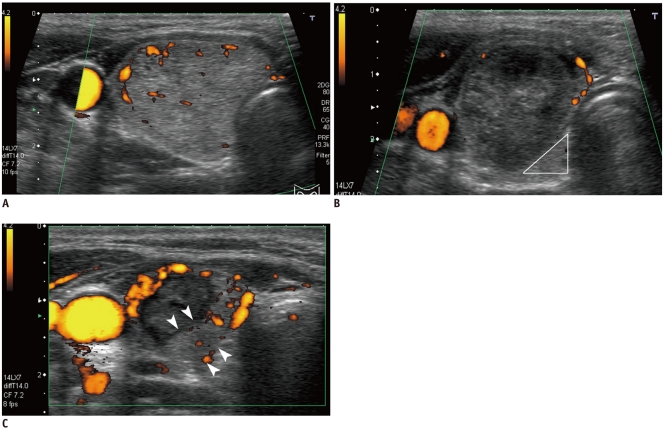
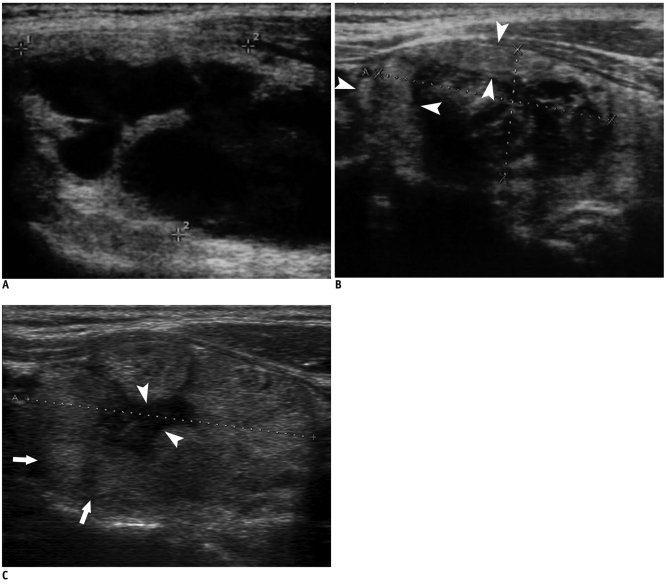
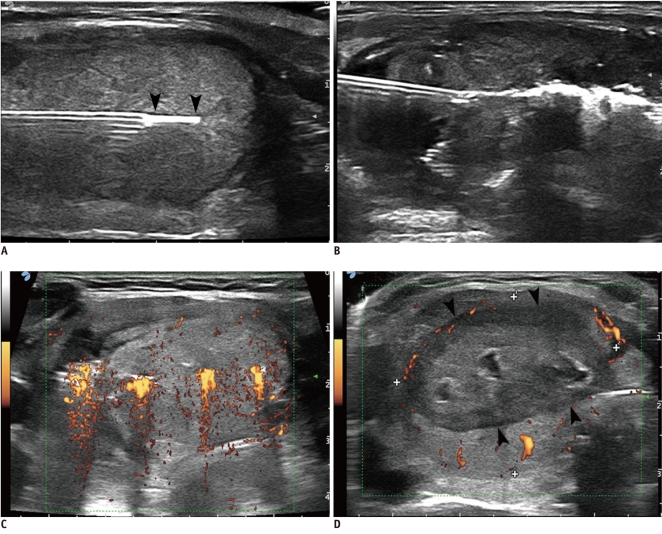
US images showing danger triangle. A. Transverse image obtained before ablation, in which right thyroid nodule fills entire right thyroid gland and lies close to trachea and recurrent laryngeal nerve. B. Transverse US image taken immediately after ablation, demonstrating less-than-adequate treatment of danger triangle (white triangle), because recurrent laryngeal nerve is located in danger triangle. C. Transverse US image taken one month after ablation, showing that undertreated portion indicated by arrowheads is now apart from recurrent laryngeal nerve and trachea, thus allowing undertreated portion to be safely ablated.
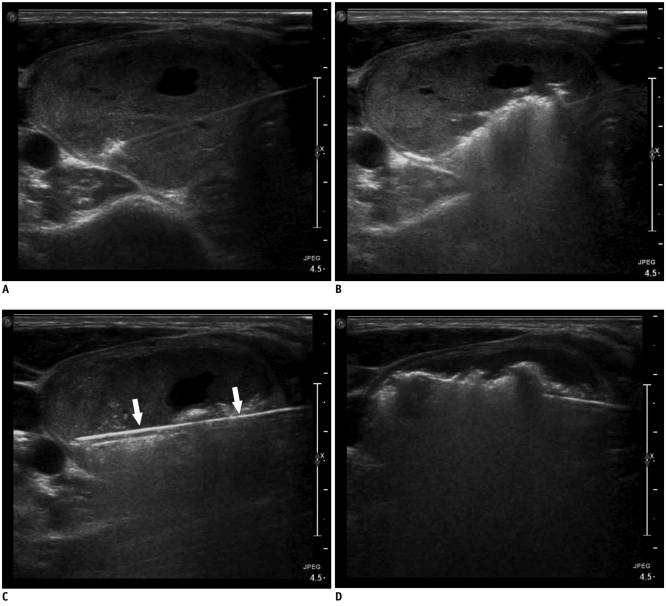
Sequential US images of moving shot technique showing complete ablation of nodule margins. A, B. Transverse US images showing initial placement of electrode at periphery of deep and remote portion of target nodule; ablation area was small at periphery and large in central safe area. C, D. Transverse US images showing re-location of electrode in untreated area. Electrode was continuously moved backward and in superficial direction within thyroid nodule. Entire length of electrode was always well demarcated (arrows).
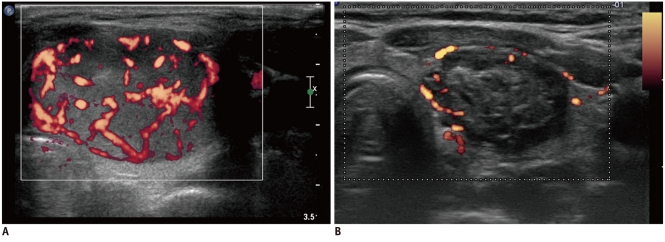
Transverse US images of well-ablated thyroid nodule, before (A) and 12 months after (B) radiofrequency ablation, showing size reduction, decreased echogenicity, and lack of internal vascularity.
Longitudinal US images showing marginal re-growth of ablated nodule. A, B. Images taken before (A) and six months after (B) radiofrequency ablation. Shrinkage of ablated thyroid nodule is evident; however, undertreated nodule margin is observed as isoechoic area (arrowheads) in contrast to well-treated central hypoechoic portion. C. Four years after radiofrequency ablation, well-treated central hypoechoic area was reduced in size (arrowheads), but marginal untreated area showed isoechoic marginal re-growth (arrows).
Transverse and longitudinal US images showing marked shrinkage of ablated nodule. Images obtained before (A, B) and 54 months after (C, D) radiofrequency ablation, showing that ablated thyroid nodule had decreased markedly in size; only small scar-like lesion remained.
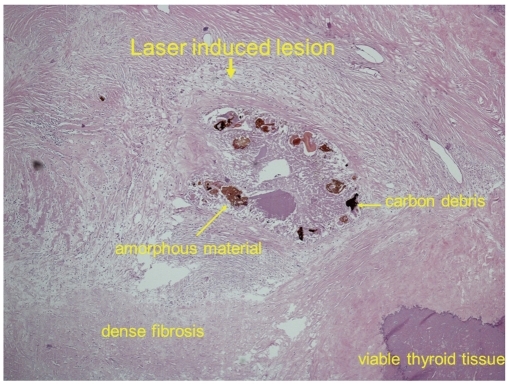
Microscopic changes occurring in benign thyroid nodule resected two years after laser ablation. Ablation zone is surrounded by peripheral rim of dense fibrous tissue. Destroyed area is represented by amorphous material, carbon debris, macrophages and/or multinucleated giant cells, and lymphocytes, with no thyroid cells. Viable tissue is visible at periphery (lower right corner), and is separated by fibrous tissue from ablation zone.
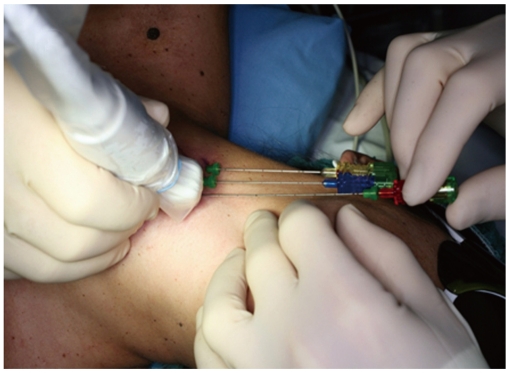
Placement of Chiba G21 needles along cranio-caudal major nodule axis; needles are separated by 10 mm.
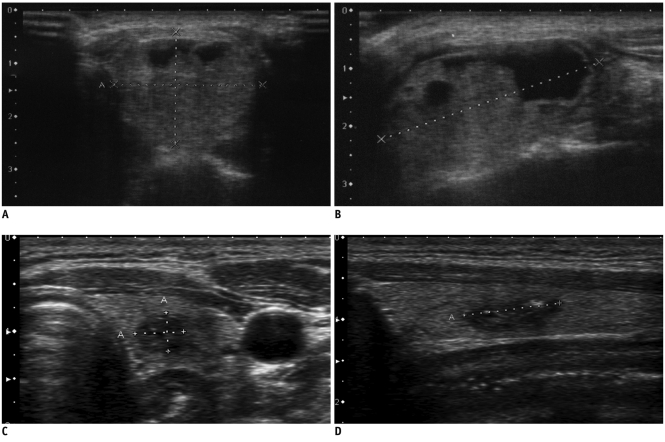
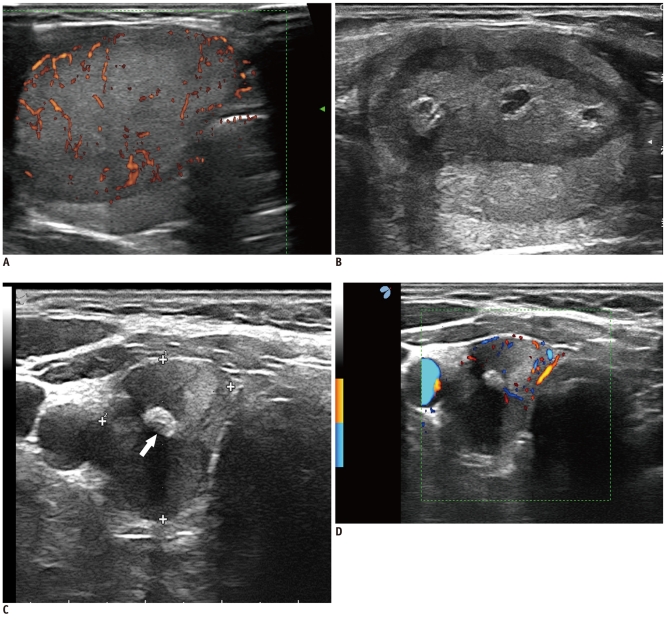
Percutaneous laser ablation procedure using three sources. A. Longitudinal US images of needle typically placed within thyroid nodule along cranio-caudal axis. Fiber is exposed to depth about 5 mm beyond tip of needle (arrowheads). B. Highly echogenic area resulting from tissue heating and vaporization is observed during laser firing. C. Color Doppler US images obtained by laser illumination. D. Final ablation: coalescence between fibers creates single lesion matching anatomy of thyroid nodule. Laser marks are seen as anechoic spots (cavitation caused by tissue vaporization) surrounded by hyperechoic rims (charring). Coagulation zone is hypoechoic parenchyma (arrowheads) separated by rim from viable tissue.
Typical three-fiber laser ablation of compact, cold, benign nodule of right thyroid lobe (volume, 25 mL). Before (A), one day after (B), one year after (C), and three years after (D) percutaneous laser ablation. Nodule shrinkage is usually associated with development of central hyperechoic area caused by tissue scarring (arrow).
References
-
- Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med. 1993;328:553–559. - PubMed
-
- Jeong WK, Baek JH, Rhim H, Kim YS, Kwak MS, Jeong HJ, et al. Radiofrequency ablation of benign thyroid nodules: safety and imaging follow-up in 236 patients. Eur Radiol. 2008;18:1244–1250. - PubMed
-
- Papini E, Guglielmi R, Bizzarri G, Pacella CM. Ultrasound-guided laser thermal ablation for treatment of benign thyroid nodules. Endocr Pract. 2004;10:276–283. - PubMed
-
- Shemen LJ, Strong EW. Complications after total thyroidectomy. Otolaryngol Head Neck Surg. 1989;101:472–475. - PubMed
-
- Papini E, Guglielmi R, Bizzarri G, Graziano F, Bianchini A, Brufani C, et al. Treatment of benign cold thyroid nodules: a randomized clinical trial of percutaneous laser ablation versus levothyroxine therapy or follow-up. Thyroid. 2007;17:229–235. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
