The Clinical Value of Performing an MRI before Prostate Biopsy
- PMID: 21927706
- PMCID: PMC3162225
- DOI: 10.4111/kju.2011.52.8.572
The Clinical Value of Performing an MRI before Prostate Biopsy
Abstract
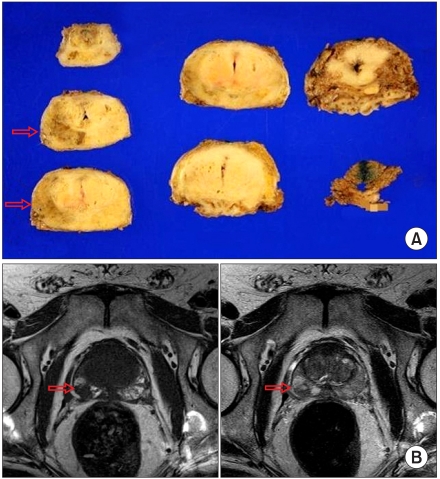
Purpose: Prostate cancer foci have a characteristic feature in magnetic resonance imaging (MRI). We aimed to assess the clinical value of MRI before prostate biopsy in prostate cancer detection.
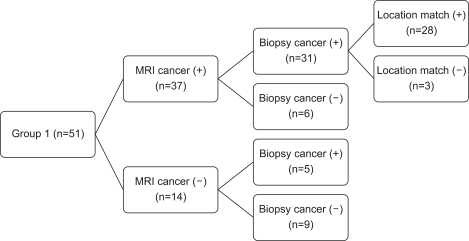
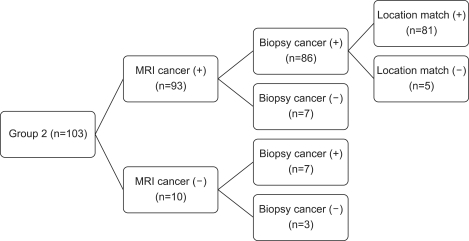
Materials and methods: From March 2009 to June 2010, 154 patients were enrolled in this study. A total of 51 patients with a clinical suspicion of prostate cancer underwent prostate MRI by a 3T scanner before transrectal ultrasound (TRUS)-guided biopsies. A total of 103 patients with a clinical suspicion of prostate cancer underwent prostate MRI after biopsies. The sensitivity, specificity, and positive predictive value (PPV) were evaluated. In addition, tumor location of pathologic findings and ADC mapping on MRI were matched and compared.
Results: The sensitivity of MRI before and after biopsy was 84.8% and 92.4%, respectively. The PPV of MRI before and after biopsy was 75.7% and 92.4%, respectively. The MRI location match percentage before and after biopsy was 89.3% and 94.1%, respectively.
Conclusions: Compared with other previous reports, our results show that the prostate cancer detection sensitivity of MRI is on the rise. Furthermore, MRI before prostate biopsy can provide more information by which to identify prostate cancer during prostate biopsy and thus reduce the false-negative rate.
Keywords: Biopsy; MRI; Prostate cancer.
Conflict of interest statement
The authors have nothing to disclose.
Figures
Similar articles
-
Multiparametric MRI in detection and staging of prostate cancer.Dan Med J. 2017 Feb;64(2):B5327. Dan Med J. 2017. PMID: 28157066 Review.
-
MRI-guided biopsy of the prostate: correlation between the cancer detection rate and the number of previous negative TRUS biopsies.Diagn Interv Radiol. 2013 Sep-Oct;19(5):411-7. doi: 10.5152/dir.2013.13055. Diagn Interv Radiol. 2013. PMID: 23886937
-
Multiparametric magnetic resonance imaging can exclude prostate cancer progression in patients on active surveillance: a retrospective cohort study.Eur Radiol. 2020 Nov;30(11):6042-6051. doi: 10.1007/s00330-020-06997-1. Epub 2020 Jun 26. Eur Radiol. 2020. PMID: 32591887 Free PMC article.
-
[MRI navigated stereotactic prostate biopsy: fusion of MRI and real-time transrectal ultrasound images for perineal prostate biopsies].Urologe A. 2012 Jan;51(1):50-6. doi: 10.1007/s00120-011-2707-3. Urologe A. 2012. PMID: 21935634 German.
-
Comparison of Magnetic Resonance Imaging-stratified Clinical Pathways and Systematic Transrectal Ultrasound-guided Biopsy Pathway for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials.Eur Urol Oncol. 2019 Nov;2(6):605-616. doi: 10.1016/j.euo.2019.05.004. Epub 2019 Jun 14. Eur Urol Oncol. 2019. PMID: 31204311 Free PMC article.
Cited by
-
Paradigm Shift in Prostate Cancer Diagnosis: Pre-Biopsy Prostate Magnetic Resonance Imaging and Targeted Biopsy.Korean J Radiol. 2022 Jun;23(6):625-637. doi: 10.3348/kjr.2022.0059. Epub 2022 May 9. Korean J Radiol. 2022. PMID: 35555886 Free PMC article. Review.
-
Comparison of bi- and multiparametric magnetic resonance imaging to select men for active surveillance.Acta Radiol Open. 2019 Jul 31;8(8):2058460119866352. doi: 10.1177/2058460119866352. eCollection 2019 Aug. Acta Radiol Open. 2019. PMID: 31392035 Free PMC article.
-
MRI-targeted prostate biopsy: a review of technique and results.Nat Rev Urol. 2013 Oct;10(10):589-97. doi: 10.1038/nrurol.2013.196. Epub 2013 Sep 24. Nat Rev Urol. 2013. PMID: 24061532 Review.
References
-
- Levi F, Lucchini F, Negri E, Boyle P, La Vecchia C. Leveling of prostate cancer mortality in Western Europe. Prostate. 2004;60:46–52. - PubMed
-
- Hayat MJ, Howlader N, Reichman ME, Edwards BK. Cancer statistics, trends, and multiple primary cancer analyses from the Surveillance, Epidemiology, and End Results (SEER) Program. Oncologist. 2007;12:20–37. - PubMed
-
- Horndalsveen Berild G, Nielsen K. Accuracy in Core Biopsy of the Prostate. An autopsy study. Urol Int. 1986;41:276–278. - PubMed
-
- Loch T, Eppelmann U, Lehmann J, Wullich B, Loch A, Stockle M. Transrectal ultrasound guided biopsy of the prostate: random sextant versus biopsies of sono-morphologically suspicious lesions. World J Urol. 2004;22:357–360. - PubMed
-
- Wefer AE, Hricak H, Vigneron DB, Coakley FV, Lu Y, Wefer J, et al. Sextant localization of prostate cancer: comparison of sextant biopsy, magnetic resonance imaging and magnetic resonance spectroscopic imaging with step section histology. J Urol. 2000;164:400–404. - PubMed
LinkOut - more resources
Full Text Sources