

Delayed graft function in the kidney transplant
- PMID: 21929642
- PMCID: PMC3280444
- DOI: 10.1111/j.1600-6143.2011.03754.x
Delayed graft function in the kidney transplant
Abstract
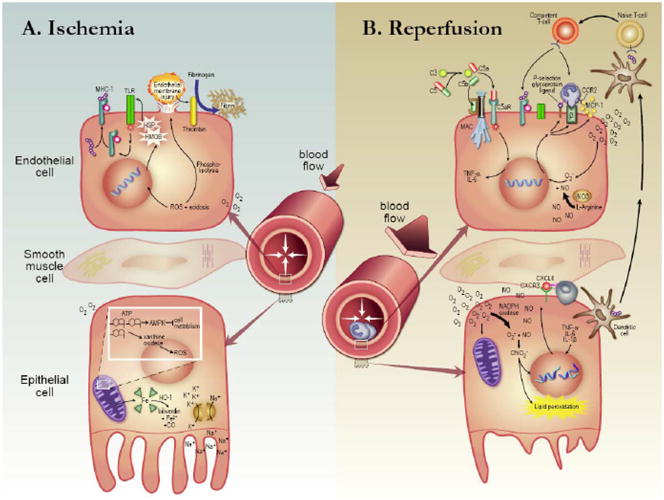
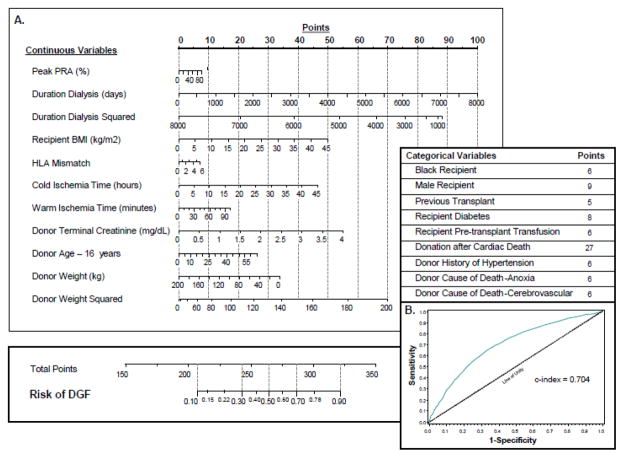
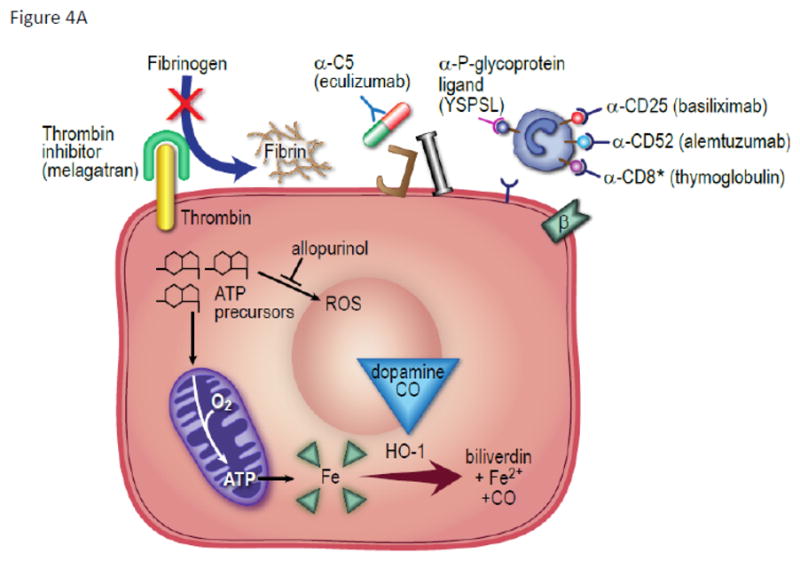
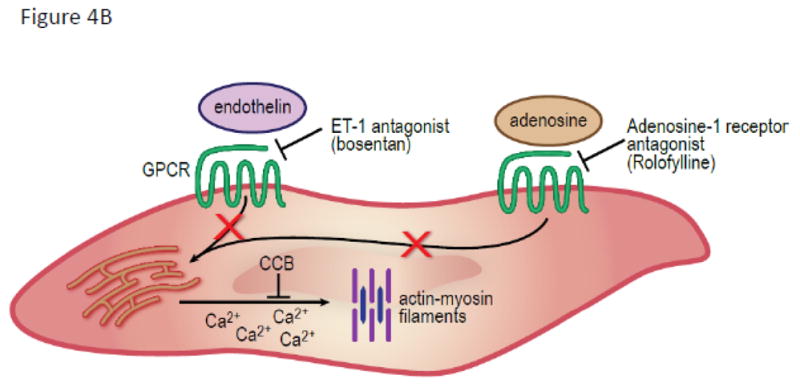
Acute kidney injury occurs with kidney transplantation and too frequently progresses to the clinical diagnosis of delayed graft function (DGF). Poor kidney function in the first week of graft life is detrimental to the longevity of the allograft. Challenges to understand the root cause of DGF include several pathologic contributors derived from the donor (ischemic injury, inflammatory signaling) and recipient (reperfusion injury, the innate immune response and the adaptive immune response). Progressive demand for renal allografts has generated new organ categories that continue to carry high risk for DGF for deceased donor organ transplantation. New therapies seek to subdue the inflammatory response in organs with high likelihood to benefit from intervention. Future success in suppressing the development of DGF will require a concerted effort to anticipate and treat tissue injury throughout the arc of the transplantation process.
©2011 The Authors Journal compilation © 2011 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the American Journal of Transplantation.
Figures

References
-
- KDIGO Nephrology Guideline Database. Available from: http://www.kdigo.org/nephrology_guideline_database/guideline_summaries_b....
-
- Chang SH, Russ GR, Chadban SJ, Campbell SB, McDonald SP. Trends in kidney transplantation in Australia and New Zealand, 1993–2004. Transplantation. 2007;84(5):611–618. - PubMed
-
- Halloran PF, Aprile MA, Farewell V, Ludwin D, Smith EK, Tsai SY, et al. Early function as the principal correlate of graft survival. A multivariate analysis of 200 cadaveric renal transplants treated with a protocol incorporating antilymphocyte globulin and cyclosporine. Transplantation. 1988;46(2):223–228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
