

Effects of vasopressinergic receptor agonists on sublingual microcirculation in norepinephrine-dependent septic shock
- PMID: 21929764
- PMCID: PMC3334762
- DOI: 10.1186/cc10453
Effects of vasopressinergic receptor agonists on sublingual microcirculation in norepinephrine-dependent septic shock
Abstract
Introduction: The present study was designed to determine the effects of continuously infused norepinephrine (NE) plus (1) terlipressin (TP) or (2) arginine vasopressin (AVP) or (3) placebo on sublingual microcirculation in septic shock patients. The primary study end point was a difference of ≥ 20% in the microvascular flow index of small vessels among groups.
Methods: The design of the study was a prospective, randomized, double-blind clinical trial. NE was titrated to maintain mean arterial pressure (MAP) between 65 and 75 mmHg after establishment of normovolemia in 60 septic shock patients. Thereafter patients (n = 20 per group) were randomized to receive continuous infusions of either TP (1 μg/kg/hour), AVP (0.04 U/minute) or placebo (isotonic saline). In all groups, open-label NE was adjusted to maintain MAP within threshold values if needed. The sublingual microcirculatory blood flow of small vessels was assessed by sidestream dark-field imaging. All measurements, including data from right heart catheterization and norepinephrine requirements, were obtained at baseline and 6 hours after randomization.
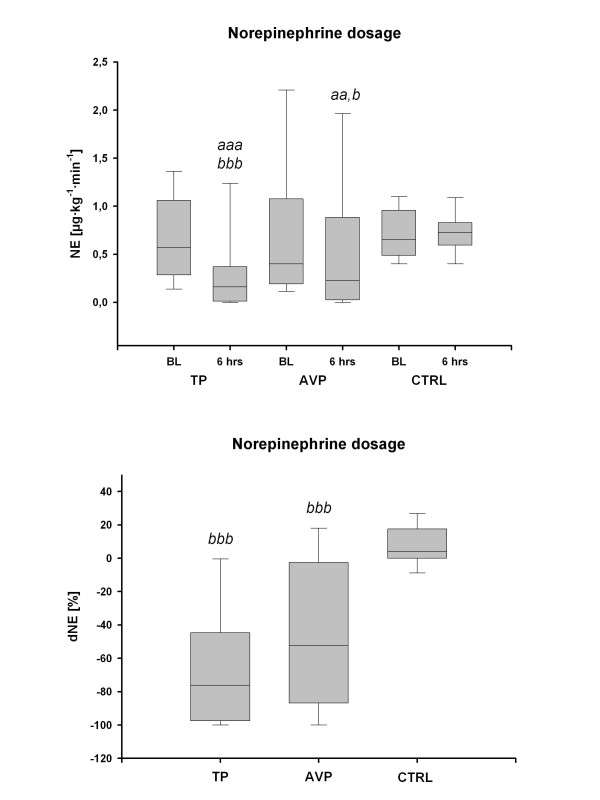
Results: TP and AVP decreased NE requirements at the end of the 6-hour study period. The data are medians (25th and 75th interquartile ranges (IQRs)): 0.57 μg/kg/minute (0.29 to 1.04) vs. 0.16 μg/kg/minute (0.03 to 0.37) for TP and 0.40 μg/kg/minute (0.20 to 1.05) vs. 0.23 μg/kg/minute (0.03 to 0.77) for AVP, with statistical significance of P < 0.05 vs. baseline and vs. placebo. There were no differences in sublingual microcirculatory variables, systemic hemodynamics, oxygen transport and acid-base homeostasis among the three study groups during the entire observation period. The proportions of perfused vessels increased in relation to baseline within all study groups, and there were no significant differences between groups. The specific data were as follows (median (IQR)): 9.7% (2.6 to 19.8) for TP, 8.9% (0.0 to 17.8) for AVP, and 6.9% (3.5 to 10.1) for placebo (P < 0.05 vs. baseline for each comparison), as well as perfused vessel density 18.6% (8.6 to 36.9) for TP, 20.2% (-3.0 to 37.2) for AVP, and 11.4% (-3.0 to 19.4) for placebo (P < 0.05 vs. baseline for each comparison).
Conclusions: The present study suggests that to achieve a MAP of 65 to 75 mmHg in septic patients treated with NE, the addition of continuously infused low-dose TP or AVP does not affect sublingual microcirculatory blood flow. In addition, our results suggest that microcirculatory flow abnormalities are mainly related to other factors (for example, volume status, timing, hemodynamics and progression of the disease) rather than to the vasopressor per se.
Trial registration: ClinicalTrial.gov NCT00995839.
Figures


References
-
- Dellinger RP, Levy MM, Carlet JM, Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. International Surviving Sepsis Campaign Guidelines Committee; American Association of Critical Care Nurses; American College of Chest Physicians; American College of Emergency Physicians; Canadian Critical Care Society; European Society of Clinical Microbiology and Infectious Diseases; European Society of Intensive Care Medicine; European Respiratory Society; International Sepsis Forum; Japanese Association for Acute Medicine; Japanese Society of Intensive Care Medicine; Society of Critical Care Medicine; Society of Hospital Medicine; Surgical Infection Society; World Federation of Societies of Intensive and Critical Care Medicine. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296–327. doi: 10.1097/01.CCM.0000298158.12101.41. - DOI - PubMed
-
- Trzeciak S, Cinel I, Phillip Dellinger R, Shapiro NI, Arnold RC, Parrillo JE, Hollenberg SM. Microcirculatory Alterations in Resuscitation and Shock (MARS) Investigators. Resuscitating the microcirculation in sepsis: the central role of nitric oxide, emerging concepts for novel therapies, and challenges for clinical trials. Acad Emerg Med. 2008;15:399–413. doi: 10.1111/j.1553-2712.2008.00109.x. - DOI - PMC - PubMed
-
- Trzeciak S, Dellinger RP, Parrillo JE, Guglielmi M, Bajaj J, Abate NL, Arnold RC, Colilla S, Zanotti S, Hollenberg SM. Microcirculatory Alterations in Resuscitation and Shock Investigators. Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: relationship to hemodynamics, oxygen transport, and survival. Ann Emerg Med. 2007;49:88–98. doi: 10.1016/j.annemergmed.2006.08.021. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
