

Outcome of extremely low birth weight infants who received delivery room cardiopulmonary resuscitation
- PMID: 21930284
- PMCID: PMC3258355
- DOI: 10.1016/j.jpeds.2011.07.041
Outcome of extremely low birth weight infants who received delivery room cardiopulmonary resuscitation
Abstract
Objective: To determine whether delivery room cardiopulmonary resuscitation (DR-CPR) independently predicts morbidities and neurodevelopmental impairment (NDI) in extremely low birth weight infants.
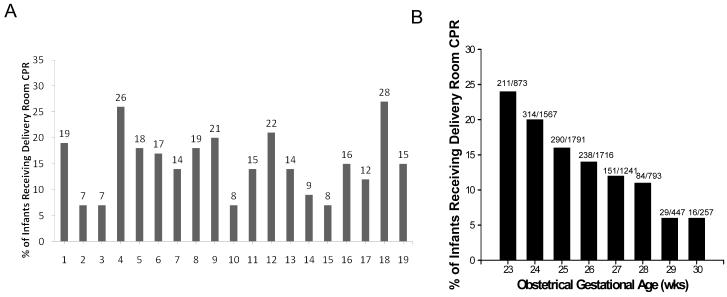
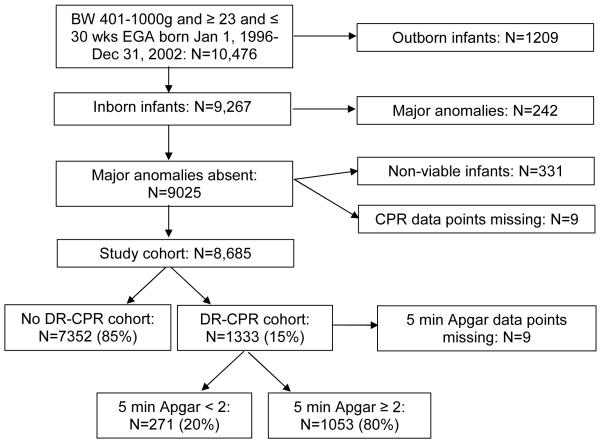
Study design: We conducted a cohort study of infants born with birth weight of 401 to 1000 g and gestational age of 23 to 30 weeks. DR-CPR was defined as chest compressions, medications, or both. Logistic regression was used to determine associations among DR-CPR and morbidities, mortality, and NDI at 18 to 24 months of age (Bayley II mental or psychomotor index <70, cerebral palsy, blindness, or deafness). Data are adjusted ORs with 95% CIs.
Results: Of 8685 infants, 1333 (15%) received DR-CPR. Infants who received DR-CPR had lower birth weight (708±141 g versus 764±146g, P<.0001) and gestational age (25±2 weeks versus 26±2 weeks, P<.0001). Infants who received DR-CPR had more pneumothoraces (OR, 1.28; 95% CI, 1.48-2.99), grade 3 to 4 intraventricular hemorrhage (OR, 1.47; 95% CI, 1.23-1.74), bronchopulmonary dysplasia (OR, 1.34; 95% CI, 1.13-1.59), death by 12 hours (OR, 3.69; 95% CI, 2.98-4.57), and death by 120 days after birth (OR, 2.22; 95% CI, 1.93-2.57). Rates of NDI in survivors (OR, 1.23; 95% CI, 1.02-1.49) and death or NDI (OR, 1.70; 95% CI, 1.46-1.99) were higher for DR-CPR infants. Only 14% of DR-CPR recipients with 5-minute Apgar score <2 survived without NDI.
Conclusions: DR-CPR is a prognostic marker for higher rates of mortality and NDI for extremely low birth weight infants. New DR-CPR strategies are needed for this population.
Copyright © 2012 Mosby, Inc. All rights reserved.
Figures
References
-
- Finer NN, Horbar JD, Carpenter JH. Cardiopulmonary resuscitation in the very low birth weight infant: the Vermont Oxford Network experience. Pediatrics. 1999;104:428–34. - PubMed
-
- Shah PS. Extensive cardiopulmonary resuscitation for VLBW and ELBW infants: a systematic review and meta-analyses. J Perinatol. 2009;29:655–61. - PubMed
-
- Vyas H, Field D, Milner AD, Hopkin IE. Determinants of the first inspiratory volume and functional residual capacity at birth. Pediatr Pulmonol. 1986;2:189–93. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- M01 RR000039/RR/NCRR NIH HHS/United States
- M01 RR000030/RR/NCRR NIH HHS/United States
- M01 RR000633/RR/NCRR NIH HHS/United States
- M01 RR000997/RR/NCRR NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- UL1 RR024139/RR/NCRR NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- U10 HD040521/HD/NICHD NIH HHS/United States
- U10 HD021415/HD/NICHD NIH HHS/United States
- M01 RR002172/RR/NCRR NIH HHS/United States
- M01 RR008084/RR/NCRR NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- M01 RR002635/RR/NCRR NIH HHS/United States
- U10 HD040461/HD/NICHD NIH HHS/United States
- M01 RR000044/RR/NCRR NIH HHS/United States
- M01 RR016587/RR/NCRR NIH HHS/United States
- M01 RR000750/RR/NCRR NIH HHS/United States
- U10 HD040689/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD021397/HD/NICHD NIH HHS/United States
- U10 HD034167/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- UL1 TR000041/TR/NCATS NIH HHS/United States
- M01 RR007122/RR/NCRR NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- M01 RR000032/RR/NCRR NIH HHS/United States
- M01 RR000070/RR/NCRR NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
- U10 HD040498/HD/NICHD NIH HHS/United States
- UG1 HD068278/HD/NICHD NIH HHS/United States
- M01 RR000125/RR/NCRR NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
