

Hospital readmissions among patients with decompensated cirrhosis
- PMID: 21931378
- PMCID: PMC3470789
- DOI: 10.1038/ajg.2011.314
Hospital readmissions among patients with decompensated cirrhosis
Abstract
Objectives: Early rehospitalizations have been well characterized in many disease states, but not among patients with cirrhosis. The aims of this study were to identify the frequency, costs, predictors, and preventable causes of hospital readmissions among patients with decompensated cirrhosis.
Methods: Rates of readmission were calculated for 402 patients discharged after one of the following complications of cirrhosis: ascites, spontaneous bacterial peritonitis, renal failure, hepatic encephalopathy, or variceal hemorrhage. Costs of readmissions were calculated using the hospital accounting system. Predictors of time to first readmission were determined using Cox regression, and predictors of hospitalization rate/person-years were determined using negative binomial regression. The independent association between readmission rate and mortality was determined using Cox regression. Admissions within 30 days of discharge were assessed by two reviewers to determine if preventable.
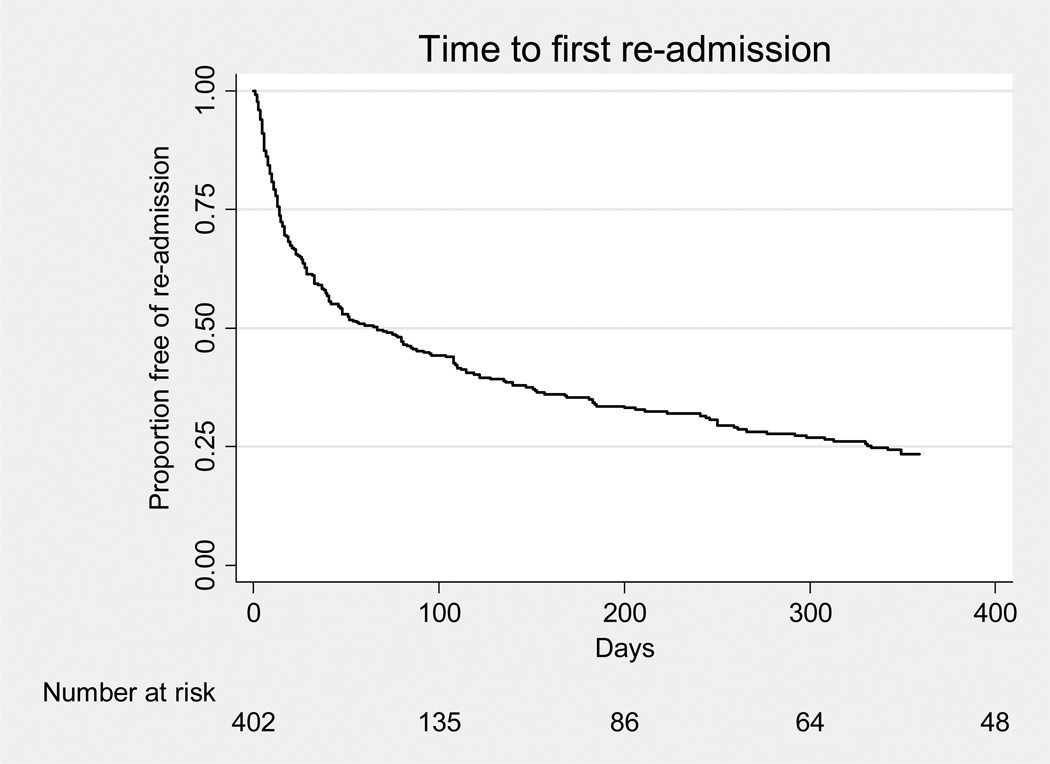
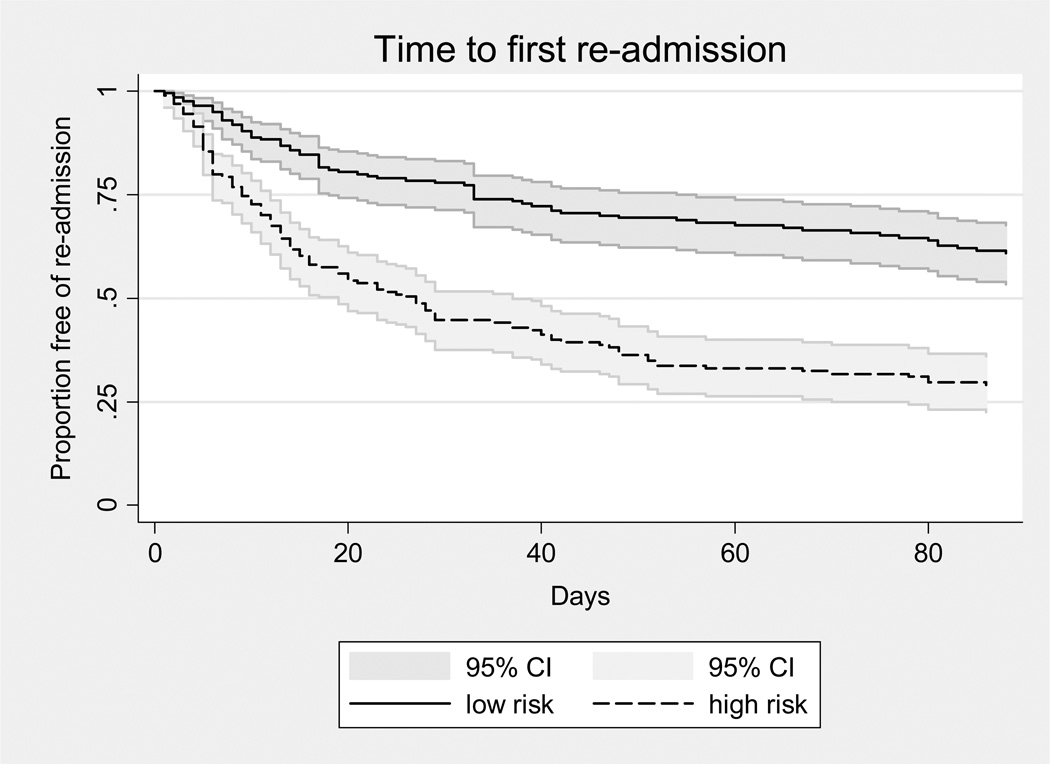
Results: Overall, 276 (69%) subjects had at least one nonelective readmission, with a median time to first readmission of 67 days. By 1 week after discharge, 14% of subjects had been readmitted, and 37% were readmitted within 1 month. The mean costs for readmissions within 1 week and between weeks 1 and 4 were $28,898 and $20,581, respectively. During a median follow-up of 203 days, the median number of readmissions was 2 (range 0-40), with an overall rate of 3 hospitalizations/person-years. Patients with more frequent readmissions had higher risk of subsequent mortality, despite adjustment for confounders including the Model for End-stage Liver Disease (MELD) score. Predictors of time to first readmission included MELD score, serum sodium, and number of medications on discharge; predictors of hospitalization rate included these variables as well as the number of cirrhosis complications and being on the transplant list at discharge. Among 165 readmissions within 30 days, 22% were possibly preventable.
Conclusions: Hospital readmissions among patients with decompensated cirrhosis are common, costly, moderately predictable, in some cases, possibly preventable, and independently associated with mortality. These findings support the development of disease management interventions to prevent rehospitalization.
Conflict of interest statement
Conflicts of interest: none of the authors has any conflict of interest for this study.
Figures
Comment in
-
Hospital Readmissions in Decompensated Cirrhosis.Am J Gastroenterol. 2015 Jun;110(6):940. doi: 10.1038/ajg.2015.142. Am J Gastroenterol. 2015. PMID: 26052778 No abstract available.
References
-
- Kim WR, Brown RS, Jr, Terrault NA, et al. Burden of liver disease in the United States: summary of a workshop. Hepatology. 2002;36:227–242. - PubMed
-
- Talwalkar JA. Prophylaxis with beta blockers as a performance measure of quality health care in cirrhosis. Gastroenterology. 2006;130:1005–1007. - PubMed
-
- Nguyen GC, Segev DL, Thuluvath PJ. Nationwide increase in hospitalizations and hepatitis C among inpatients with cirrhosis and sequelae of portal hypertension. Clin Gastroenterol Hepatol. 2007;5:1092–1099. - PubMed
-
- Institute of Medicine (U.S.) Crossing the quality chasm : a new health system for the 21st century. Washington, D.C.: National Academy Press; 2001. Committee on Quality of Health Care in America. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
