

Calcineurin-inhibitor minimization in liver transplant patients with calcineurin-inhibitor-related renal dysfunction: a meta-analysis
- PMID: 21931704
- PMCID: PMC3170329
- DOI: 10.1371/journal.pone.0024387
Calcineurin-inhibitor minimization in liver transplant patients with calcineurin-inhibitor-related renal dysfunction: a meta-analysis
Abstract
Background: Introduction of calcineurin-inhibitor (CNI) has made transplantation a miracle in the past century. However, the side effects of long-term use of CNI turn out to be one of the major challenges in the current century. Among these, renal dysfunction attracts more and more attention. Herein, we undertook a meta-analysis to evaluate the efficacy and safety of calcineurin-inhibitor (CNI) minimization protocols in liver transplant recipients with CNI-related renal dysfunction.
Methods: We included randomized trials with no year and language restriction. All data were analyzed using random effect model by Review Manager 5.0. The primary endpoints were glomerular filtration rate (GFR), serum creatinine level (sCr) and creatinine clearance rate (CrCl), and the secondary endpoints were acute rejection episodes, incidence of infection and patient survival at the end of follow-up.
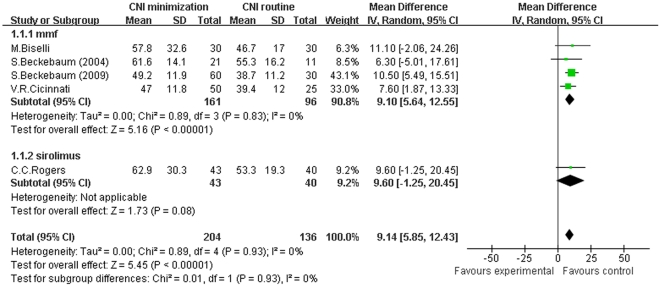
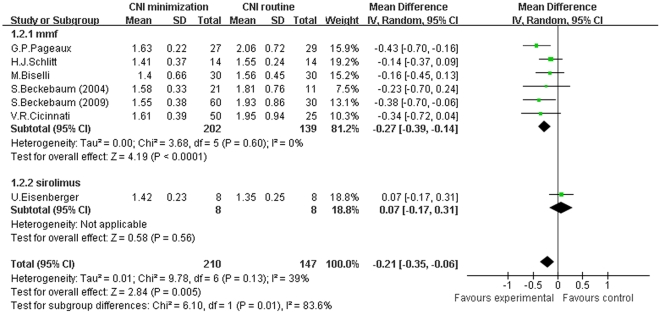
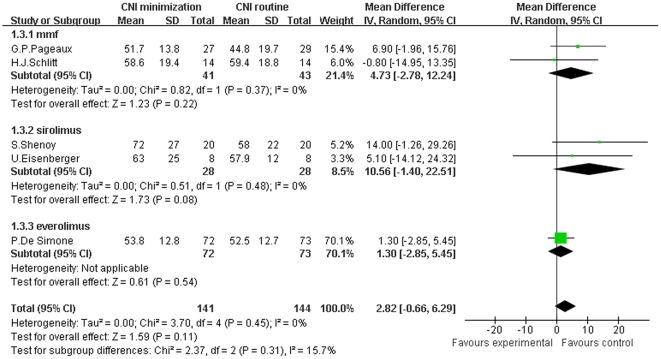
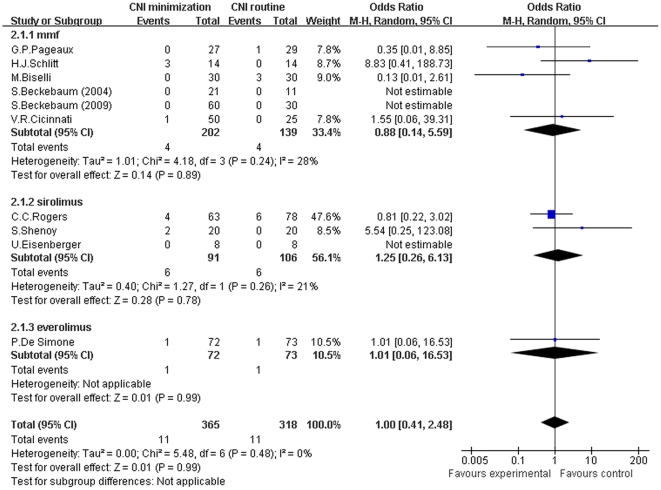
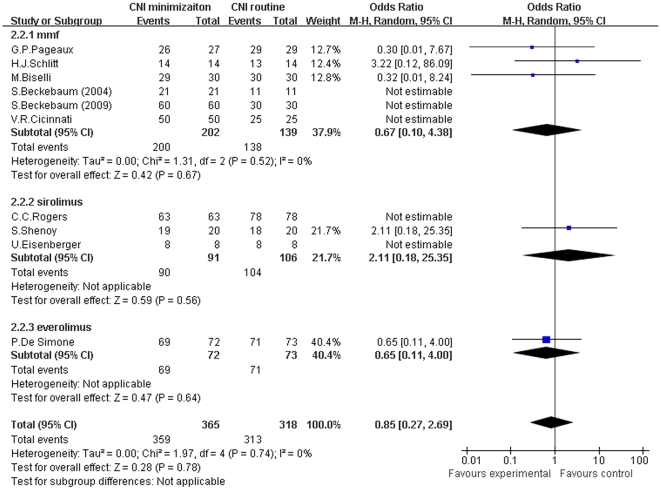
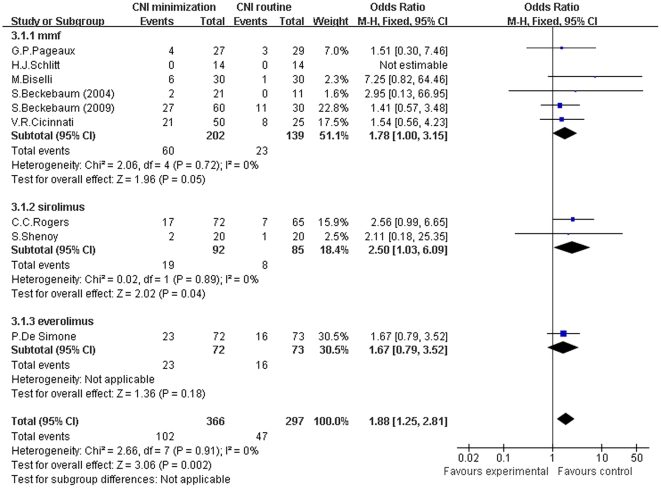
Results: GFR was significantly improved in CNI minimization group than in routine CNI regimen group (Z = 5.45, P<0.00001; I(2) = 0%). Likely, sCr level was significantly lower in the CNI minimization group (Z = 2.84, P = 0.005; I(2) = 39%). However, CrCl was not significantly higher in the CNI minimization group (Z = 1.59, P = 0.11; I(2) = 0%). Both acute rejection episodes and patient survival were comparable between two groups (rejection: Z = 0.01, P = 0.99; I(2) = 0%; survival: Z = 0.28, P = 0.78; I(2) = 0%, respectively). However, current CNI minimization protocols may be related to a higher incidence of infections (Z = 3.06, P = 0.002; I(2) = 0%).
Conclusion: CNI minimization can preserve or even improve renal function in liver transplant patients with renal impairment, while sharing similar short term acute rejection rate and patient survival with routine CNI regimen.
Conflict of interest statement
Figures
References
-
- Organ Procurement and Transplant Network. Available: http://optn.transplant.hrsa.gov/LatestData/viewDataReports.asp via the Internet. Accessed June 2011.
-
- Ojo AO, Held PJ, Port FK, Wolfe RA, Leichtman AB, et al. Chronic renal failure after transplantation of a nonrenal organ. N Engl J Med. 2003;349:931–940. - PubMed
-
- Lebron Gallardo M, Herrera Gutierrez ME, Seller Perez G, Curiel Balsera E, Fernandez Ortega JF, et al. Risk factors for renal dysfunction in the postoperative course of liver transplant. Liver Transpl. 2004;11:1379–1385. - PubMed
-
- Pawarode A, Fine DM, Thuluwath PJ. Independent risk factors and natural history of renal dysfunction in liver transplant recipients. Liver Transpl. 2003;9:741–747. - PubMed
-
- Moreno JM, Cuervas-Mons V, Rubio E, Pons F, Herreros de TA, et al. Chronic renal dysfunction after liver transplantation in adult patients: prevalence, risk factors, and impact on mortality. Transplant Proc. 2003;35:1907–1908. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
