

An integrated randomized intervention to reduce behavioral and psychosocial risks: pregnancy and neonatal outcomes
- PMID: 21931956
- PMCID: PMC3288486
- DOI: 10.1007/s10995-011-0875-9
An integrated randomized intervention to reduce behavioral and psychosocial risks: pregnancy and neonatal outcomes
Abstract
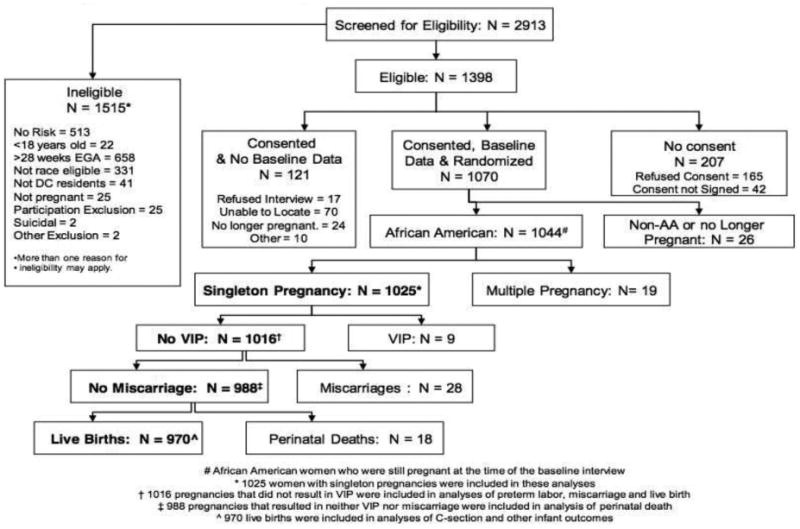
While biomedical risks contribute to poor pregnancy and neonatal outcomes in African American (AA) populations, behavioral and psychosocial risks (BPSR) may also play a part. Among low income AA women with psychosocial risks, this report addresses the impacts on pregnancy and neonatal outcomes of an integrated education and counseling intervention to reduce BPSR, as well as the contributions of other psychosocial and biomedical risks. Subjects were low income AA women ≥18 years living in the Washington, DC, metropolitan area and seeking prenatal care. Subjects (n = 1,044) were screened for active smoking, environmental tobacco smoke exposure (ETSE), depression, or intimate partner violence (IPV) and then randomized to intervention (IG) or usual care (UCG) groups. Data were collected prenatally, at delivery, and postpartum by maternal report and medical record abstraction. Multiple imputation methodology was used to estimate missing variables. Rates of pregnancy outcomes (miscarriage, live birth, perinatal death), preterm labor, Caesarean section, sexually transmitted infection (STI) during pregnancy, preterm birth (<37 weeks), low birth weight (<2,500 g), very low birth weight (<1,500 g), small for gestational age, neonatal intensive care unit (NICU) admission, and >2 days of hospitalization were compared between IG and UCG. Logistic regression models were created to predict outcomes based on biomedical risk factors and the four psychosocial risks (smoking, ETSE, depression, and IPV) targeted by the intervention. Rates of adverse pregnancy and neonatal outcomes were high and did not differ significantly between IG and UCG. In adjusted analysis, STI during the current pregnancy was associated with IPV (OR = 1.41, 95% CI 1.04-1.91). Outcomes such as preterm labor, caesarian section in pregnancy and preterm birth, low birth weight, small for gestational age, NICU admissions and >2 day hospitalization of the infants were associated with biomedical risk factors including preexisting hypertension and diabetes, previous preterm birth (PTB), and late initiation of prenatal care, but they were not significantly associated with active smoking, ETSE, depression, or IPV. Neither the intervention to reduce BPSR nor the psychosocial factors significantly contributed to the pregnancy and neonatal outcomes. This study confirms that biomedical factors significantly contribute to adverse outcomes in low income AA women. Biomedical factors outweighed psychosocial factors in contributing to adverse pregnancy and neonatal outcomes in this high-risk population. Early identification and management of hypertension, diabetes and previous PTB in low income AA women may reduce health disparities in birth outcomes. Level of evidence I.
Figures
References
-
- MacDorman MF, Callaghan WM, Mathews TJ, Hoyert DL, Kochanek KD. Trends in preterm-related infant mortality by race and ethnicity, United States, 1999-2004. International Jouranl of Health Services. 2007;37(4):635–41. - PubMed
-
- Paul DA, Mackley A, Locke RG, Stefano JL, Kroelinger C. State infant mortality: an ecologic study to determine modifiable risks and adjusted infant mortality rates. Maternal Child Health Journal. 2009;13(3):343–8. - PubMed
-
- SCHSA. SCHSA State Center for Health Statistics Administration: Briefing paper on the 2000 infant mortality rate for the District of Columbia. 2002.
-
- Mathews TJ, MacDorman MF. Infant mortality statistics from the 2005 period linked birth/infant death data set. National Vital Statistics Report. 2008;57(2):1–32. - PubMed
-
- Nothnagle M, Marchi K, Egerter S, Braveman P. Risk factors for late or no prenatal care following Medicaid expansions in California. Maternal Child Health Journal. 2000;4(4):251–9. - PubMed
Publication types
MeSH terms
Grants and funding
- 5U18HD31206/HD/NICHD NIH HHS/United States
- 3U18HD030447/HD/NICHD NIH HHS/United States
- U18 HD031919/HD/NICHD NIH HHS/United States
- U10 HD047890/HD/NICHD NIH HHS/United States
- U18 HD030447/HD/NICHD NIH HHS/United States
- U18 HD036104/HD/NICHD NIH HHS/United States
- 3U18HD030445/HD/NICHD NIH HHS/United States
- U10 HD030445/HD/NICHD NIH HHS/United States
- 5U18HD036104/HD/NICHD NIH HHS/United States
- U18 HD031206/HD/NICHD NIH HHS/United States
- U18 HD030445/HD/NICHD NIH HHS/United States
- 3U18HD031919/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
