

Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis
- PMID: 21933749
- PMCID: PMC3328296
- DOI: 10.1016/S1470-2045(11)70232-7
Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis
Abstract
Background: ALK gene rearrangement defines a new molecular subtype of non-small-cell lung cancer (NSCLC). In a recent phase 1 clinical trial, the ALK tyrosine-kinase inhibitor (TKI) crizotinib showed marked antitumour activity in patients with advanced, ALK-positive NSCLC. To assess whether crizotinib affects overall survival in these patients, we did a retrospective study comparing survival outcomes in crizotinib-treated patients in the trial and crizotinib-naive controls screened during the same time period.
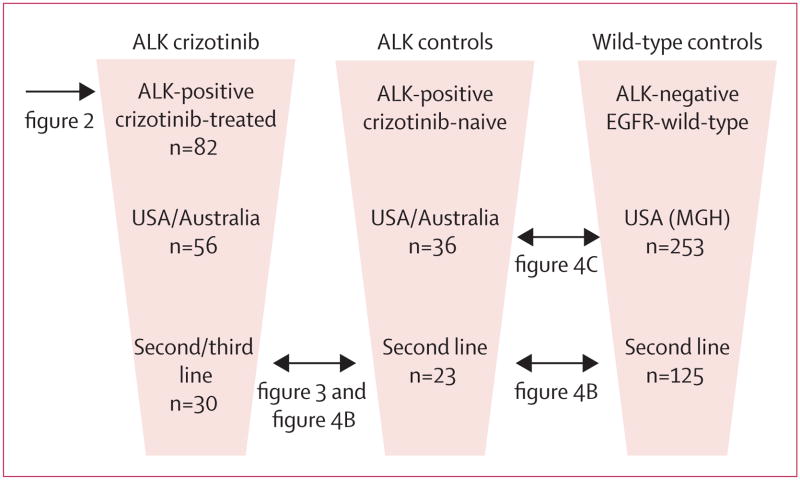
Methods: We examined overall survival in patients with advanced, ALK-positive NSCLC who enrolled in the phase 1 clinical trial of crizotinib, focusing on the cohort of 82 patients who had enrolled through Feb 10, 2010. For comparators, we identified 36 ALK-positive patients from trial sites who were not given crizotinib (ALK-positive controls), 67 patients without ALK rearrangement but positive for EGFR mutation, and 253 wild-type patients lacking either ALK rearrangement or EGFR mutation. To assess differences in overall survival, we assessed subsets of clinically comparable ALK-positive and ALK-negative patients.
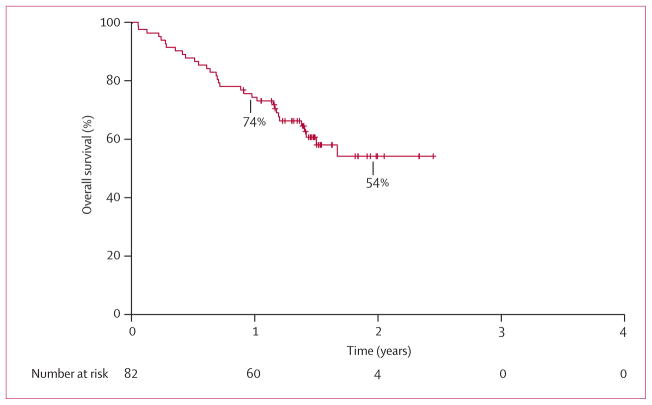
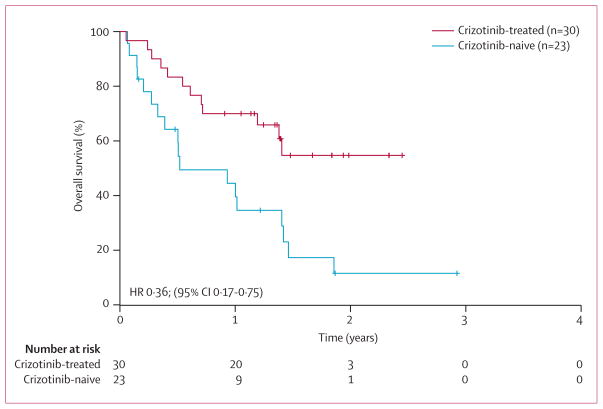
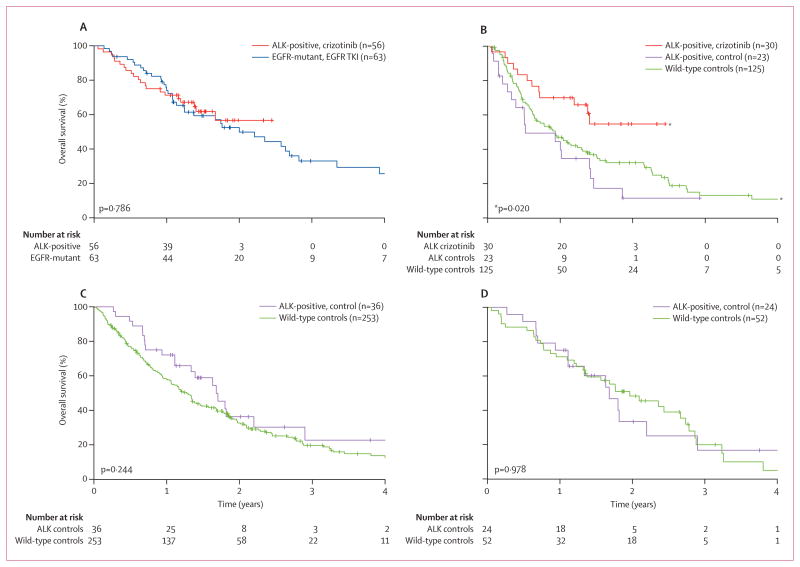
Findings: Among 82 ALK-positive patients who were given crizotinib, median overall survival from initiation of crizotinib has not been reached (95% CI 17 months to not reached); 1-year overall survival was 74% (95% CI 63-82), and 2-year overall survival was 54% (40-66). Overall survival did not differ based on age, sex, smoking history, or ethnic origin. Survival in 30 ALK-positive patients who were given crizotinib in the second-line or third-line setting was significantly longer than in 23 ALK-positive controls given any second-line therapy (median overall survival not reached [95% CI 14 months to not reached] vs 6 months [4-17], 1-year overall survival 70% [95% CI 50-83] vs 44% [23-64], and 2-year overall survival 55% [33-72] vs 12% [2-30]; hazard ratio 0·36, 95% CI 0·17-0·75; p=0·004). Survival in 56 crizotinib-treated, ALK-positive patients was similar to that in 63 ALK-negative, EGFR-positive patients given EGFR TKI therapy (median overall survival not reached [95% CI 17 months to not reached] vs 24 months [15-34], 1-year overall survival 71% [95% CI 58-81] vs 74% [61-83], and 2-year overall survival 57% [40-71] vs 52% [38-65]; p=0·786), whereas survival in 36 crizotinib-naive, ALK-positive controls was similar to that in 253 wild-type controls (median overall survival 20 months [95% CI 13-26] vs 15 months [13-17]; p=0·244).
Interpretation: In patients with advanced, ALK-positive NSCLC, crizotinib therapy is associated with improved survival compared with that of crizotinib-naive controls. ALK rearrangement is not a favourable prognostic factor in advanced NSCLC.
Funding: Pfizer Inc, V Foundation for Cancer Research.
Trial registration: ClinicalTrials.gov NCT00585195.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Conflict of interest statement
ATS, BJS, DBC, RGM, Y-JB, ELK, and AJI received honoraria or consulting fees from Pfizer. RGM served as a paid expert witness for Pfizer. BJS, GJR, GIS, RGM, and Y-JB received research funding from Pfizer. KK, PS, YT, and KDW are employees and stockholders of Pfizer. AJI received honoraria or consulting fees from Abbott Laboratories. ATS, GJR, JAE, and JWC received honoraria or consulting fees from ARIAD. ATS and GJR received honoraria or consulting fees from Chugai. GJR received honoraria or consulting fees from Merck, Boehringer-Ingelheim, and Tragara. JAE received consulting fees and research funding from Novartis and AstraZeneca. All other authors declared no conflicts of interest.
Figures
Comment in
-
Hope without hype: EML4-ALK inhibition for treatment of lung cancer.Lancet Oncol. 2011 Oct;12(11):983-4. doi: 10.1016/S1470-2045(11)70253-4. Epub 2011 Sep 18. Lancet Oncol. 2011. PMID: 21933750 No abstract available.
References
-
- Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448:561–66. - PubMed
-
- Rikova K, Guo A, Zeng Q, et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer. Cell. 2007;131:1190–203. - PubMed
-
- Wong DW, Leung EL, So KK, et al. The EML4-ALK fusion gene is involved in various histologic types of lung cancers from nonsmokers with wild-type EGFR and KRAS. Cancer. 2009;115:1723–33. - PubMed
-
- Takeuchi K, Choi YL, Soda M, et al. Multiplex reverse transcription-PCR screening for EML4-ALK fusion transcripts. Clin Cancer Res. 2008;14:6618–24. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
