

Significant reduction of red blood cell transfusion requirements by changing from a double-unit to a single-unit transfusion policy in patients receiving intensive chemotherapy or stem cell transplantation
- PMID: 21933858
- PMCID: PMC3248939
- DOI: 10.3324/haematol.2011.047035
Significant reduction of red blood cell transfusion requirements by changing from a double-unit to a single-unit transfusion policy in patients receiving intensive chemotherapy or stem cell transplantation
Abstract
Background: Traditionally, single-unit red blood cell transfusions were believed to be insufficient to treat anemia, but recent data suggest that they may lead to a safe reduction of transfusion requirements. We tested this hypothesis by changing from a double- to a single-unit red blood cell transfusion policy.
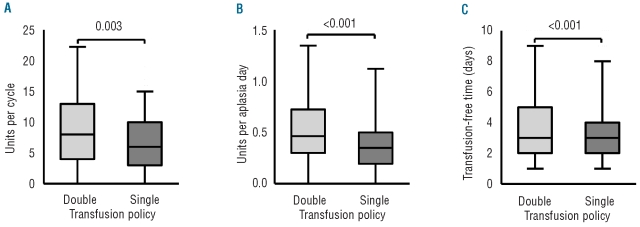
Design and methods: We performed a retrospective cohort study in patients with hematologic malignancies receiving intensive chemotherapy or hematopoietic stem cell transplantation. The major end-points were the reduction in the total number of red blood cell units per therapy cycle and per day of aplasia. The study comprised 139 patients who received 272 therapy cycles. Overall 2212 red blood cell units were administered in 1548 transfusions.
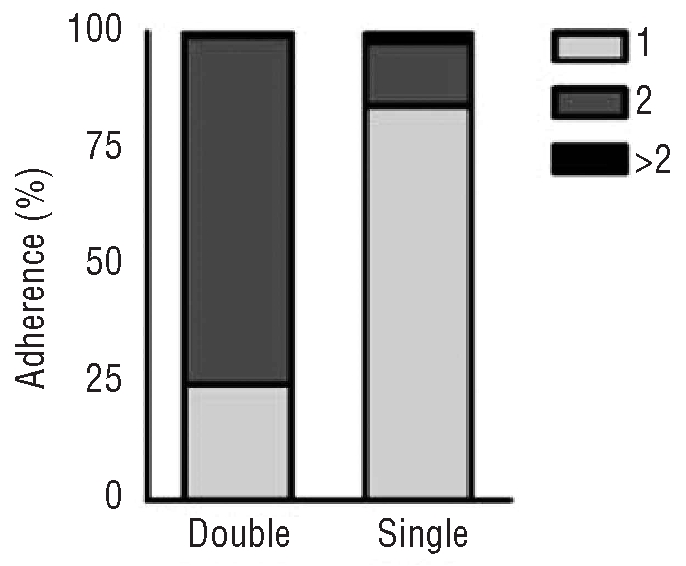
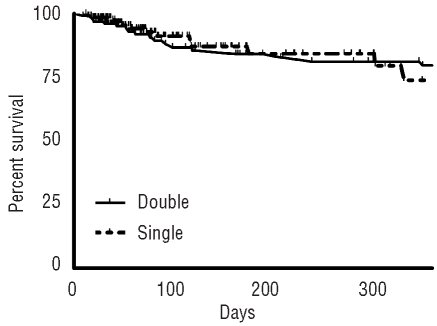
Results: During the periods of the double- and single-unit policies, one red blood cell unit was transfused in 25% and 84% of the cases and the median number of red blood cell units per transfusion was two and one, respectively. Single-unit transfusion led to a 25% reduction of red blood cell usage per therapy cycle and 24% per aplasia day, but was not associated with a higher out-patient transfusion frequency. In multivariate analysis, single-unit transfusion resulted in a reduction of 2.7 red blood cell units per treatment cycle (P = 0.001). The pre-transfusion hemoglobin levels were lower during the single-unit period (median 61 g/L versus 64 g/L) and more transfusions were administered to patients with hemoglobin values of 60 gl/L or less (47% versus 26%). There was no evidence of more severe bleeding or more platelet transfusions during the single-unit period and the overall survival was similar in both cohorts.
Conclusions: Implementing a single-unit transfusion policy saves 25% of red blood cell units and, thereby, reduces the risks associated with allogeneic blood transfusions.
Figures
Comment in
-
Single versus double-unit transfusion policy in hematology.Haematologica. 2012 Jul;97(7):e25. doi: 10.3324/haematol.2012.065516. Haematologica. 2012. PMID: 22798546 Free PMC article. No abstract available.
References
-
- Graham-Stewart C, Lond MB. A clinical survey of blood-transfusion. Lancet. 1960;2(7147):421–4. - PubMed
-
- Alsever JB. The blood bank and homologous serum jaundice: a review of medicolegal considerations. N Engl J Med. 1959;261:383–6. - PubMed
-
- Morton JH. Surgical transfusion practices, 1967. Surgery. 1969;65(3):407–16. - PubMed
-
- Crispen JF. The single-unit transfusion. A continuing problem. Pa Med. 1966;69(1):44–8. - PubMed
-
- Reece RL, Beckett RS. Epidemiology of single-unit transfusion. A one-year experience in a community hospital. JAMA. 1966;195(10):801–16. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
