

Integrated NY-ESO-1 antibody and CD8+ T-cell responses correlate with clinical benefit in advanced melanoma patients treated with ipilimumab
- PMID: 21933959
- PMCID: PMC3189057
- DOI: 10.1073/pnas.1110814108
Integrated NY-ESO-1 antibody and CD8+ T-cell responses correlate with clinical benefit in advanced melanoma patients treated with ipilimumab
Abstract
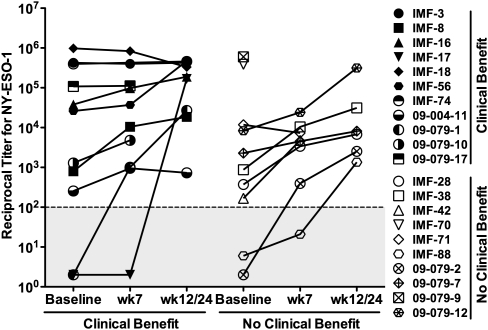
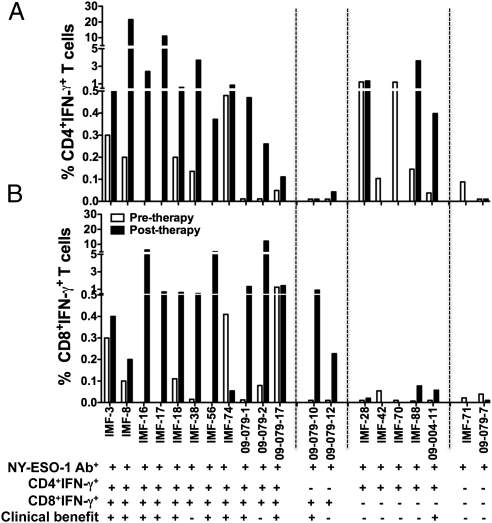
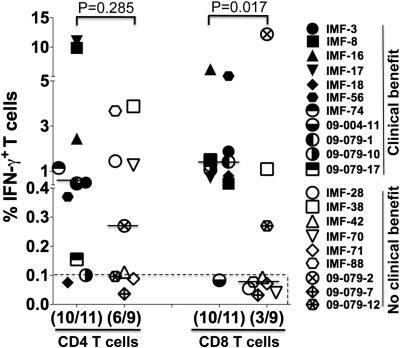
Ipilimumab, a monoclonal antibody against cytotoxic T lymphocyte antigen 4 (CTLA-4), has been shown to improve survival in patients with advanced metastatic melanoma. It also enhances immunity to NY-ESO-1, a cancer/testis antigen expressed in a subset of patients with melanoma. To characterize the association between immune response and clinical outcome, we first analyzed NY-ESO-1 serum antibody by ELISA in 144 ipilimumab-treated patients with melanoma and found 22 of 140 (16%) seropositive at baseline and 31 of 144 (22%) seropositive following treatment. These NY-ESO-1-seropositive patients had a greater likelihood of experiencing clinical benefit 24 wk after ipilimumab treatment than NY-ESO-1-seronegative patients (P = 0.02, relative risk = 1.8, two-tailed Fisher test). To understand why some patients with NY-ESO-1 antibody failed to experience clinical benefit, we analyzed NY-ESO-1-specific CD4(+) and CD8(+) T-cell responses by intracellular multicytokine staining in 20 NY-ESO-1-seropositive patients and found a surprising dissociation between NY-ESO-1 antibody and CD8 responses in some patients. NY-ESO-1-seropositive patients with associated CD8(+) T cells experienced more frequent clinical benefit (10 of 13; 77%) than those with undetectable CD8(+) T-cell response (one of seven; 14%; P = 0.02; relative risk = 5.4, two-tailed Fisher test), as well as a significant survival advantage (P = 0.01; hazard ratio = 0.2, time-dependent Cox model). Together, our data suggest that integrated NY-ESO-1 immune responses may have predictive value for ipilimumab treatment and argue for prospective studies in patients with established NY-ESO-1 immunity. The current findings provide a strong rationale for the clinical use of modulators of immunosuppression with concurrent approaches to favor tumor antigen-specific immune responses, such as vaccines or adoptive transfer, in patients with cancer.
Conflict of interest statement
Conflict of interest statement: J.P.A. and J.D.W. are paid consultants to Bristol-Myers Squibb. J.P.A. is the primary inventor on the patent “Blockade of T lymphocyte down-regulation associated with CTLA-4 signaling.”
Figures

References
-
- Boon T, Coulie PG, Van den Eynde BJ, van der Bruggen P. Human T cell responses against melanoma. Annu Rev Immunol. 2006;24:175–208. - PubMed
-
- Wang RF, Rosenberg SA. Human tumor antigens for cancer vaccine development. Immunol Rev. 1999;170:85–100. - PubMed
-
- Preuss KD, Zwick C, Bormann C, Neumann F, Pfreundschuh M. Analysis of the B-cell repertoire against antigens expressed by human neoplasms. Immunol Rev. 2002;188:43–50. - PubMed
-
- Gnjatic S, et al. NY-ESO-1: Review of an immunogenic tumor antigen. Adv Cancer Res. 2006;95:1–30. - PubMed
-
- Old LJ. Cancer vaccines: An overview. Cancer Immun. 2008;8(suppl 1):1. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
