

Clinical and demographic factors associated with antipyretic use in gram-negative severe sepsis and septic shock
- PMID: 21934034
- PMCID: PMC3517906
- DOI: 10.1345/aph.1Q319
Clinical and demographic factors associated with antipyretic use in gram-negative severe sepsis and septic shock
Abstract
Background: Antipyretic therapy is commonly prescribed for patients with infection, but studies of its impact on clinical outcomes have yielded mixed results. No data exist to characterize the use of antipyretic medications in patients with severe sepsis or septic shock.
Objective: To identify clinical and demographic factors associated with antipyretic medication administration in severe sepsis and septic shock.
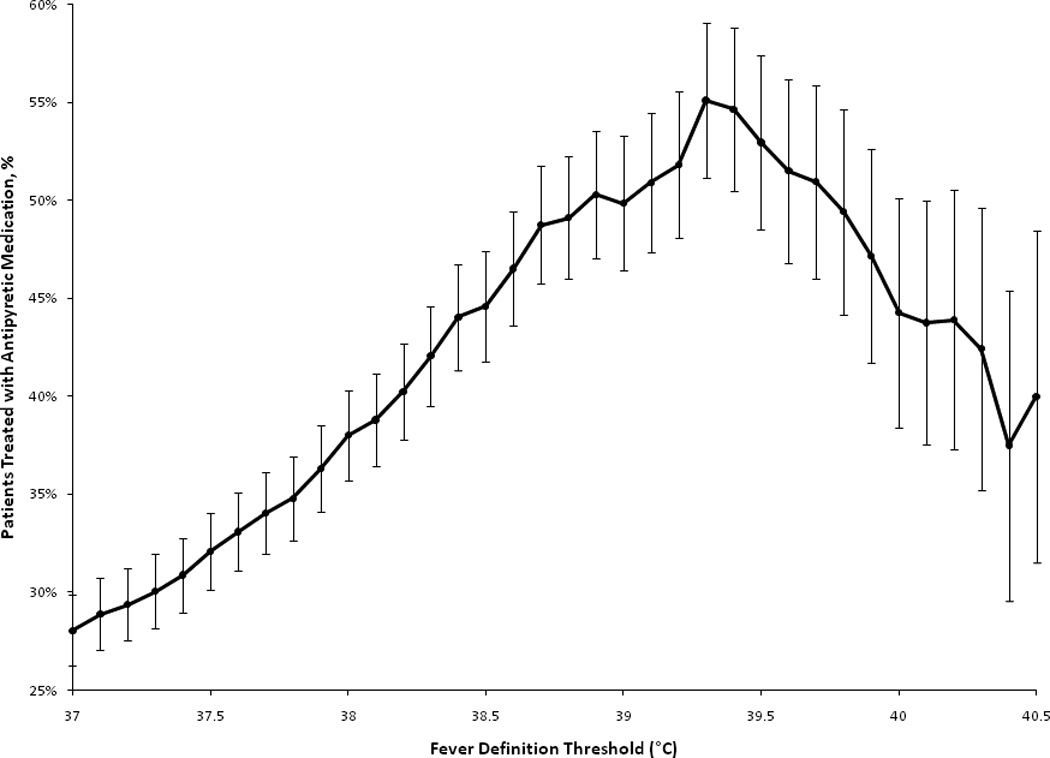
Methods: This single-center, retrospective, cohort study assessed febrile patients (temperature ≥ 38.3 °C) with gram-negative severe sepsis or septic shock at an 1111-bed academic medical center between January 2002 and February 2008. Patients were excluded if they had liver disease, acute brain injury, or allergy to acetaminophen. Generalized estimating equations were used to estimate the effect of clinical factors on treatment of patients with antipyretic medications.
Results: Although 76% of patients in this febrile cohort (n = 241) were prescribed an antipyretic agent, only 42% received antipyretic therapy; 95% of the doses were acetaminophen. Variables associated with antipyretic treatment were maximum body temperature (OR 2.11, 95% CI 1.53 to 2.89), time after sepsis diagnosis (OR 0.88, 95% CI 0.82 to 0.95), surgery during hospitalization (OR 0.49, 95% CI 0.31 to 0.80), death within 36 hours (OR 0.35, 95% CI 0.15 to 0.85), and mechanical ventilation (OR 0.58, 95% CI 0.34 to 0.98). Severity of illness factors, demographic factors, and patient treatment location did not predict who would receive antipyretic therapy.
Conclusions: Most febrile episodes in patients with gram-negative severe sepsis or septic shock were not treated with antipyretic medications. Further studies are needed to demonstrate the effect of antipyretics on clinically relevant outcomes in severe sepsis and septic shock.
Conflict of interest statement
The authors report that they have no conflicts of interest.
Figures


References
-
- Isaacs SN, Axelrod PI, Lorber B. Antipyretic orders in a university hospital. Am J Med. 1990;88(1):31–35. - PubMed
-
- Laupland KB, Shahpori R, Kirkpatrick AW, Ross T, Gregson DB, Stelfox HT. Occurrence and outcome of fever in critically ill adults. Crit Care Med. 2008;36(5):1531–1535. - PubMed
-
- Plaisance KI, Kudaravalli S, Wasserman SS, Levine MM, Mackowiak PA. Effect of antipyretic therapy on the duration of illness in experimental influenza A, Shigella sonnei, and Rickettsia rickettsii infections. Pharmacotherapy. 2000;20(12):1417–1422. - PubMed
-
- Prymula R, Siegrist CA, Chlibek R, et al. Effect of prophylactic paracetamol administration at time of vaccination on febrile reactions and antibody responses in children: two open-label, randomised controlled trials. Lancet. 2009;374(9698):1339–1350. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
