

Combined rapid (TUBEX) test for typhoid-paratyphoid A fever based on strong anti-O12 response: design and critical assessment of sensitivity
- PMID: 21935450
- PMCID: PMC3174194
- DOI: 10.1371/journal.pone.0024743
Combined rapid (TUBEX) test for typhoid-paratyphoid A fever based on strong anti-O12 response: design and critical assessment of sensitivity
Abstract
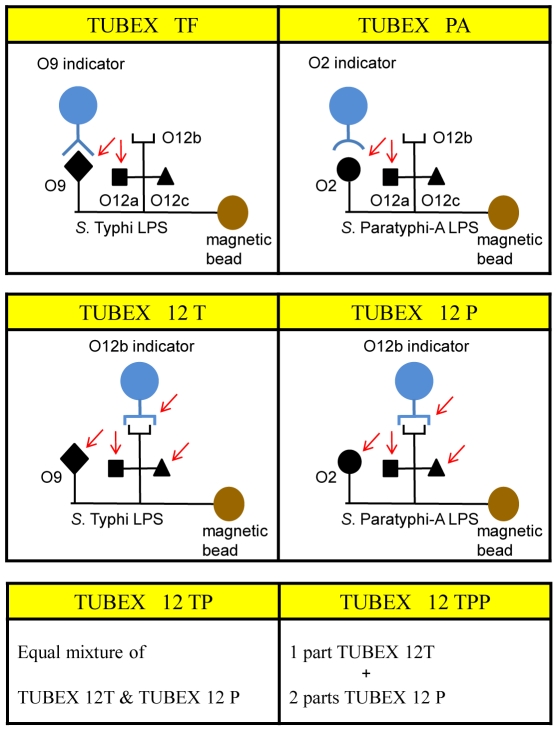
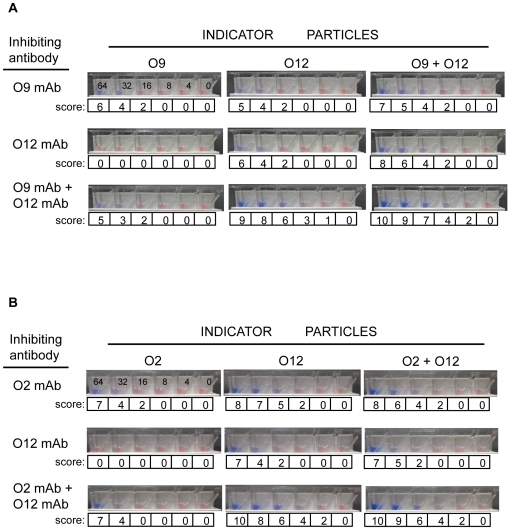
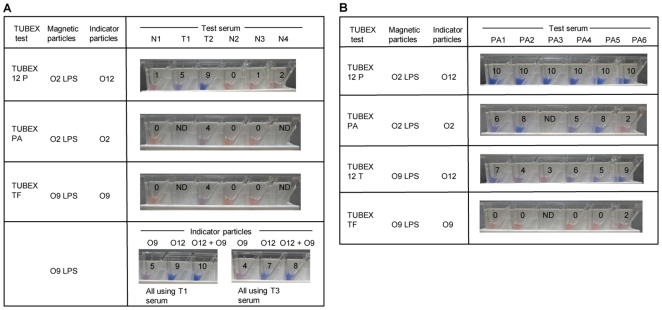
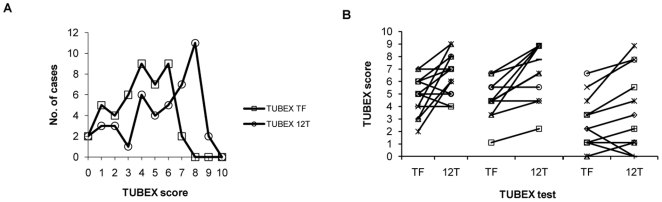
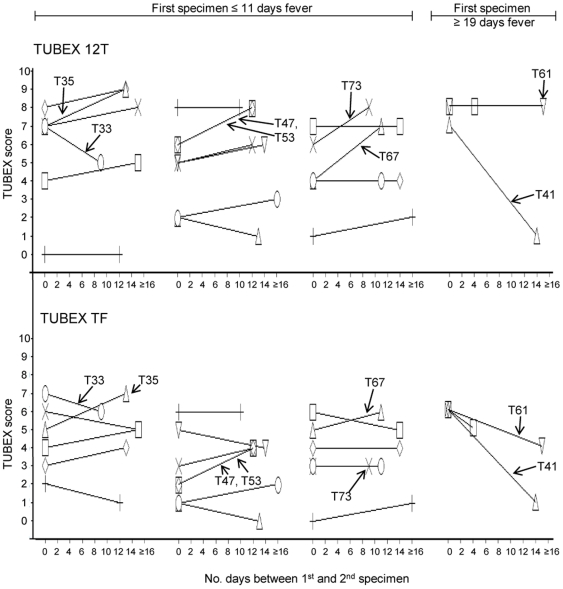
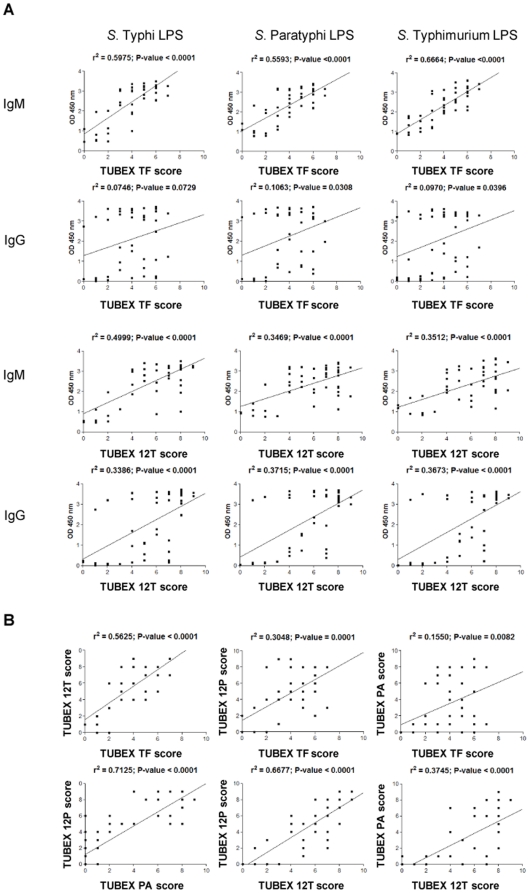
Rapid diagnostics can be accurate but, often, those based on antibody detection for infectious diseases are unwittingly underrated for various reasons. Herein, we described the development of a combined rapid test for two clinically-indistinguishable bacterial diseases, typhoid and paratyphoid A fever, the latter fast emerging as a global threat. By using monoclonal antibodies (mAbs) to bacterial antigens of known chemical structures as probes, we were able to dissect the antibody response in patients at the level of monosaccharides. Thus, a mAb specific for a common lipopolysaccharide antigen (O12) found in both the causative organisms was employed to semi-quantify the amounts of anti-O12 antibodies present in both types of patients in an epitope-inhibition particle-based (TUBEX) immunoassay. This colorimetric assay detected not only anti-O12 antibodies that were abundantly produced, but also, by steric hindrance, antibodies to an adjoining epitope (O9 or O2 in the typhoid or paratyphoid bacillus, respectively). Sensitivity and, particularly, reaction intensities, were significantly better than those obtained using an anti-O9 or anti-O2 mAb-probe in the examination of paired sera from 22 culture-confirmed typhoid patients (sensitivity, 81.8% vs 75.0%) or single sera from 36 culture-confirmed paratyphoid patients (52.8% vs 28.6), respectively. Importantly, sensitivity was better (97.1% for typhoid, 75.0% for paratyphoid) if allowance was made for the absence of relevant antibodies in certain specimens as determined by an independent, objective assay (ELISA)--such specimens might have been storage-denatured (especially the older paratyphoid samples) or procured from non-responders. Benchmarking against ELISA, which revealed high concordance between the two tests, was useful and more appropriate than comparing with culture methods as traditionally done, since antibody tests and culture target slightly different stages of these diseases. Paired sera analysis was insightful, revealing 64% of typhoid patients who had no change in antibody titer over 4-16 days, and 14% with no IgM-IgG class-switching.
Conflict of interest statement
Figures
References
-
- Widal F. Serodiagnostique de la fievre typhoid. La Semaine Medicale. 1896;259
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
