

Annual screening strategies in BRCA1 and BRCA2 gene mutation carriers: a comparative effectiveness analysis
- PMID: 21935911
- PMCID: PMC3245774
- DOI: 10.1002/cncr.26424
Annual screening strategies in BRCA1 and BRCA2 gene mutation carriers: a comparative effectiveness analysis
Erratum in
- Cancer. 2012 Nov 1;118(21):5448
Abstract
Background: Although breast cancer screening with mammography and magnetic resonance imaging (MRI) is recommended for breast cancer-susceptibility gene (BRCA) mutation carriers, there is no current consensus on the optimal screening regimen.
Methods: The authors used a computer simulation model to compare 6 annual screening strategies (film mammography [FM], digital mammography [DM], FM and magnetic resonance imaging [MRI] or DM and MRI contemporaneously, and alternating FM/MRI or DM/MRI at 6-month intervals) beginning at ages 25 years, 30 years, 35 years, and 40 years, and 2 strategies of annual MRI with delayed alternating DM/FM versus clinical surveillance alone. Strategies were evaluated without and with mammography-induced breast cancer risk using 2 models of excess relative risk. Input parameters were obtained from the medical literature, publicly available databases, and calibration.
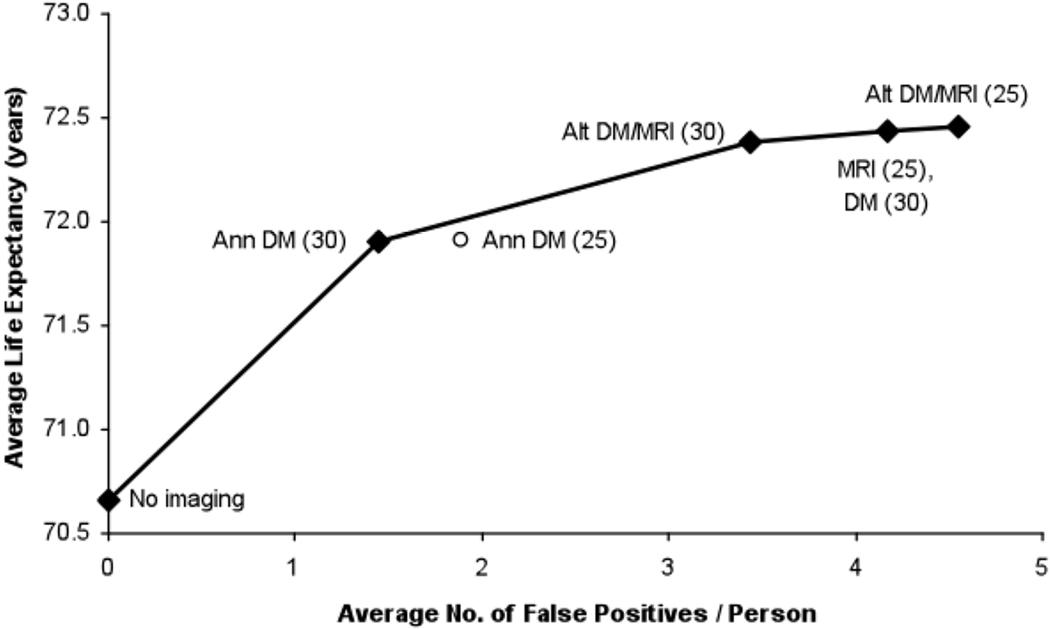
Results: Without radiation risk effects, alternating DM/MRI starting at age 25 years provided the highest life expectancy (BRCA1, 72.52 years, BRCA2, 77.63 years). When radiation risk was included, a small proportion of diagnosed cancers was attributable to radiation exposure (BRCA1, <2%; BRCA2, <4%). With radiation risk, alternating DM/MRI at age 25 years or annual MRI at age 25 years/delayed alternating DM at age 30 years was the most effective, depending on the radiation risk model used. Alternating DM/MRI starting at age 25 years also produced the highest number of false-positive screens per woman (BRCA1, 4.5 BRCA2, 8.1).
Conclusions: Annual MRI at age 25 years/delayed alternating DM at age 30 years is probably the most effective screening strategy in BRCA mutation carriers. Screening benefits, associated risks, and personal acceptance of false-positive results should be considered in choosing the optimal screening strategy for individual women.
Copyright © 2011 American Cancer Society.
Conflict of interest statement
There is no direct conflict with the content of this article.
Figures







Similar articles
-
Cost-effectiveness of alternating magnetic resonance imaging and digital mammography screening in BRCA1 and BRCA2 gene mutation carriers.Cancer. 2013 Mar 15;119(6):1266-76. doi: 10.1002/cncr.27864. Epub 2012 Nov 26. Cancer. 2013. PMID: 23184400 Free PMC article.
-
Cancer screening with digital mammography for women at average risk for breast cancer, magnetic resonance imaging (MRI) for women at high risk: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(3):1-55. Epub 2010 Mar 1. Ont Health Technol Assess Ser. 2010. PMID: 23074406 Free PMC article.
-
Cost-effectiveness of screening BRCA1/2 mutation carriers with breast magnetic resonance imaging.JAMA. 2006 May 24;295(20):2374-84. doi: 10.1001/jama.295.20.2374. JAMA. 2006. PMID: 16720823
-
Breast cancer screening of pregnant and breastfeeding women with BRCA mutations.Breast Cancer Res Treat. 2017 Apr;162(2):225-230. doi: 10.1007/s10549-017-4122-y. Epub 2017 Jan 30. Breast Cancer Res Treat. 2017. PMID: 28138892 Review.
-
Dynamic contrast-enhanced magnetic resonance imaging for risk-stratified screening in women with BRCA mutations or high familial risk for breast cancer: are we there yet?Breast Cancer Res Treat. 2020 Sep;183(2):243-250. doi: 10.1007/s10549-020-05759-3. Epub 2020 Jul 3. Breast Cancer Res Treat. 2020. PMID: 32621252 Review.
Cited by
-
Why the Gold Standard Approach by Mammography Demands Extension by Multiomics? Application of Liquid Biopsy miRNA Profiles to Breast Cancer Disease Management.Int J Mol Sci. 2019 Jun 13;20(12):2878. doi: 10.3390/ijms20122878. Int J Mol Sci. 2019. PMID: 31200461 Free PMC article. Review.
-
A Scoping Review on Calibration Methods for Cancer Simulation Models.Med Decis Making. 2025 Aug 11:272989X251353211. doi: 10.1177/0272989X251353211. Online ahead of print. Med Decis Making. 2025. PMID: 40790869 Free PMC article. Review.
-
The Breast Cancer Screening and Timing of Breast MRI-Experience in a Genetic High-Risk Screening Clinic in a Comprehensive Cancer Center.Curr Oncol. 2022 Mar 19;29(3):2119-2131. doi: 10.3390/curroncol29030171. Curr Oncol. 2022. PMID: 35323371 Free PMC article.
-
Breast care.Breast Care (Basel). 2012 Dec;7(6):501-4. doi: 10.1159/000345902. Breast Care (Basel). 2012. PMID: 24715835 Free PMC article. No abstract available.
-
"High-Risk Breast Cancer Screening in BRCA1/2 Carriers Leads to Early Detection and Improved Survival After a Breast Cancer Diagnosis".Front Oncol. 2021 Sep 2;11:683656. doi: 10.3389/fonc.2021.683656. eCollection 2021. Front Oncol. 2021. PMID: 34540661 Free PMC article.
References
-
- Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA: A Cancer Journal for Clinicians. 2007;57:75–89. - PubMed
-
- Ernestos B, Nikolaos P, Koulis G, et al. Increased chromosomal radiosensitivity in women carrying BRCA1/BRCA2 mutations assessed with the G2 assay. International Journal of Radiation Oncology, Biology, Physics. 2010;76:1199–1205. - PubMed
-
- Jansen-van der Weide MC, Greuter MJW, Jansen L, Oosterwijk JC, Pijnappel RM, de Bock GH. Exposure to low-dose radiation and the risk of breast cancer among women with a familial or genetic predisposition: a meta-analysis. European Radiology. 2010;20:2547–2556. - PubMed
-
- Berrington de Gonzalez A, Berg CD, Visvanathan K, Robson M. Estimated risk of radiation-induced breast cancer from mammographic screening for young BRCA mutation carriers. Journal of the National Cancer Institute. 2009;101:205–209. - PubMed
Publication types
MeSH terms
Grants and funding
- K07CA128816/CA/NCI NIH HHS/United States
- K25 CA133141/CA/NCI NIH HHS/United States
- U01CA69976/CA/NCI NIH HHS/United States
- U01CA63736/CA/NCI NIH HHS/United States
- U01CA86082/CA/NCI NIH HHS/United States
- U01CA86076/CA/NCI NIH HHS/United States
- R00 CA126147/CA/NCI NIH HHS/United States
- HHSN261201100031C/CA/NCI NIH HHS/United States
- K25CA133141/CA/NCI NIH HHS/United States
- U01CA70040/CA/NCI NIH HHS/United States
- U01CA63740/CA/NCI NIH HHS/United States
- U01CA70013/CA/NCI NIH HHS/United States
- R00CA126147/CA/NCI NIH HHS/United States
- K07 CA128816/CA/NCI NIH HHS/United States
- U01CA63731/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
