

Conditional survival in patients with pancreatic ductal adenocarcinoma resected with curative intent
- PMID: 21935914
- PMCID: PMC3578343
- DOI: 10.1002/cncr.26553
Conditional survival in patients with pancreatic ductal adenocarcinoma resected with curative intent
Abstract
Background: Prognosis after surgery for pancreatic ductal adenocarcinoma (PDAC) is typically reported from the date of surgery. Survival estimates, however, are dynamic and may change based on the time already survived. The authors sought to assess conditional survival among a large cohort of patients who underwent resection of PDAC.
Methods: Between 1970 and 2008, 1822 patients who underwent resection for PDAC with curative intent were identified. Kaplan-Meier and Cox regression analyses were performed to validate established predictors of survival, and results were compared with 2-year conditional survival.
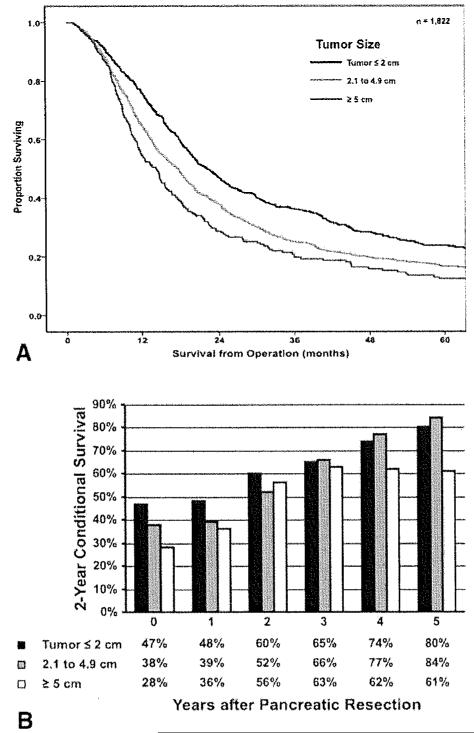
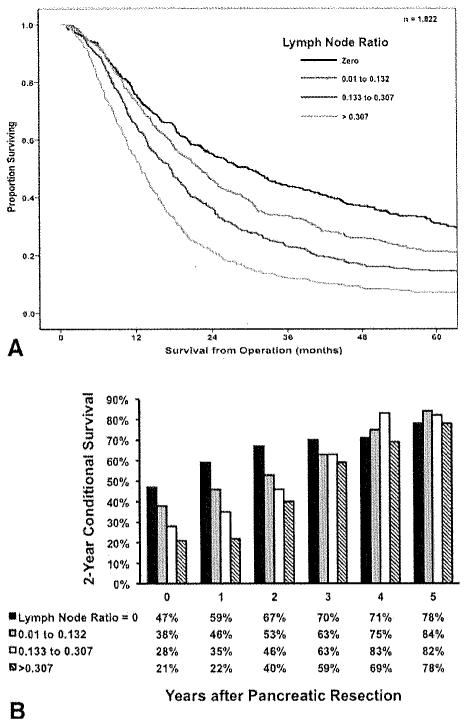
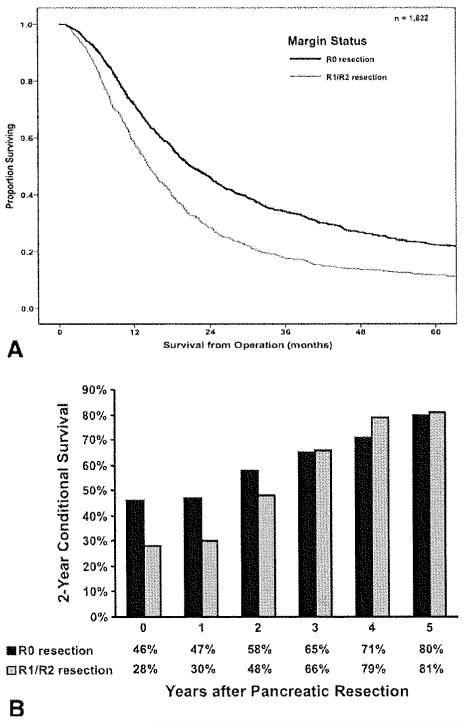
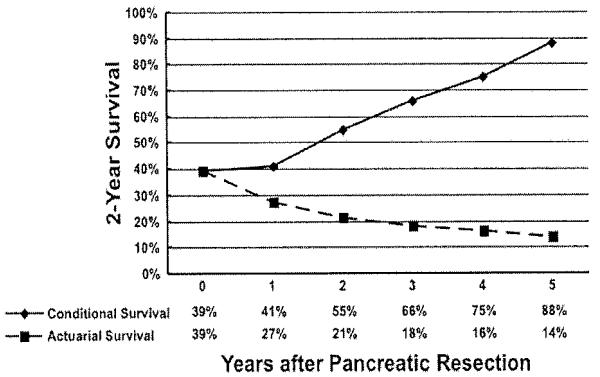
Results: Actuarial survival was 18% at 5 years, with a median survival of 18 months. Multivariate analysis revealed that tumor size, lymph node ratio, and positive margins were associated with worse survival (all P < .001). Differences in actuarial versus conditional survival estimates were greater the more years already survived by the patient. The 2-year conditional survival at 3 years-the probability of surviving to postoperative year 5 given that the patient had already survived 3 years-was 66% versus a 5-year actuarial survival calculated from the time of surgery of 18%. Stratification of 2-year conditional survival by lymph node ratio and margin status revealed that patients with high lymph node ratio or positive margins saw the greatest increase in 2-year conditional survival as more time elapsed (both P ≤ .01).
Conclusions: Differences in actuarial versus conditional survival estimates were more pronounced based on the additional years already survived by the patient. Conditional survival may be a helpful tool in counseling patients with PDAC, as it is a more accurate assessment of future survival for those patients who have already survived a certain amount of time.
Copyright © 2011 American Cancer Society.
Figures
References
-
- Jemal A, Siegel R, Xu J. Ward E. Cancer statistics. CA Cancer J Clin. 2010;2010;60:277–300. - PubMed
-
- Neoptolemos JP, Stocken DD, Friess H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004;350:1200–1210. - PubMed
-
- Oettle H, Post S, Neuhaus P, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297:267–277. - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocarcinoma of the pancreas—616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–579. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
