

Migraine attacks the Basal Ganglia
- PMID: 21936901
- PMCID: PMC3192678
- DOI: 10.1186/1744-8069-7-71
Migraine attacks the Basal Ganglia
Abstract
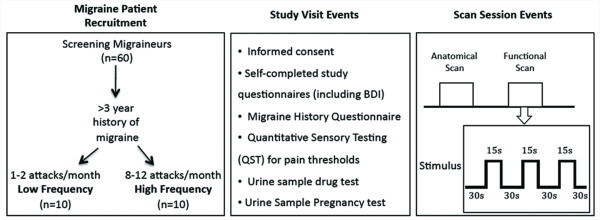
Background: With time, episodes of migraine headache afflict patients with increased frequency, longer duration and more intense pain. While episodic migraine may be defined as 1-14 attacks per month, there are no clear-cut phases defined, and those patients with low frequency may progress to high frequency episodic migraine and the latter may progress into chronic daily headache (> 15 attacks per month). The pathophysiology of this progression is completely unknown. Attempting to unravel this phenomenon, we used high field (human) brain imaging to compare functional responses, functional connectivity and brain morphology in patients whose migraine episodes did not progress (LF) to a matched (gender, age, age of onset and type of medication) group of patients whose migraine episodes progressed (HF).
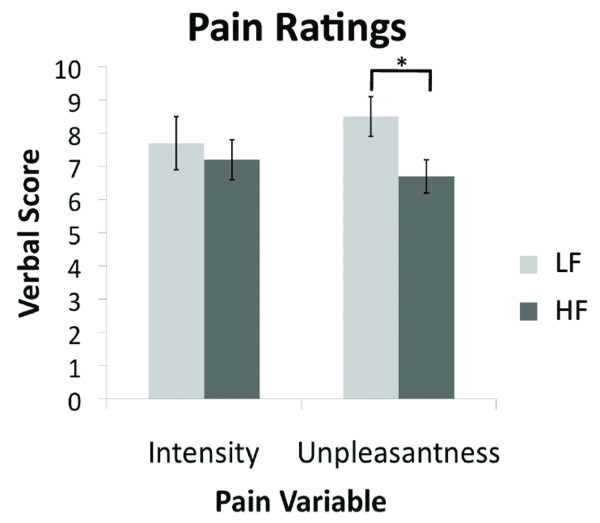
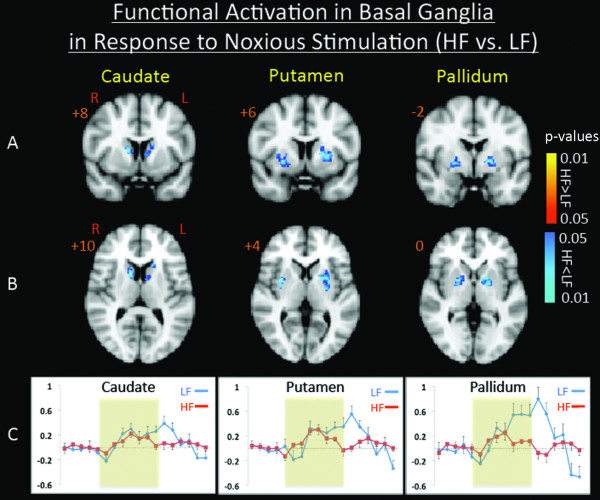
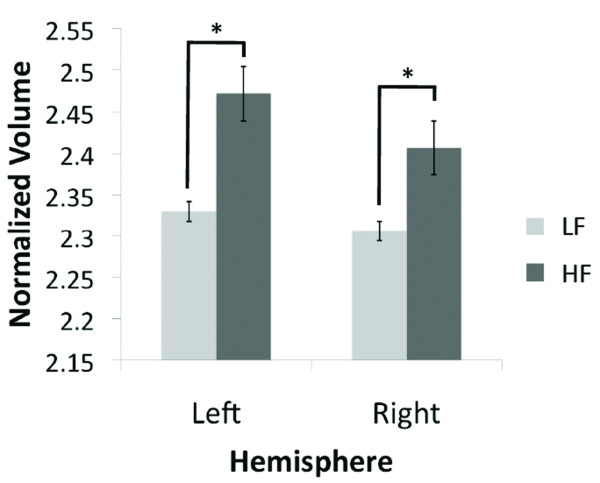
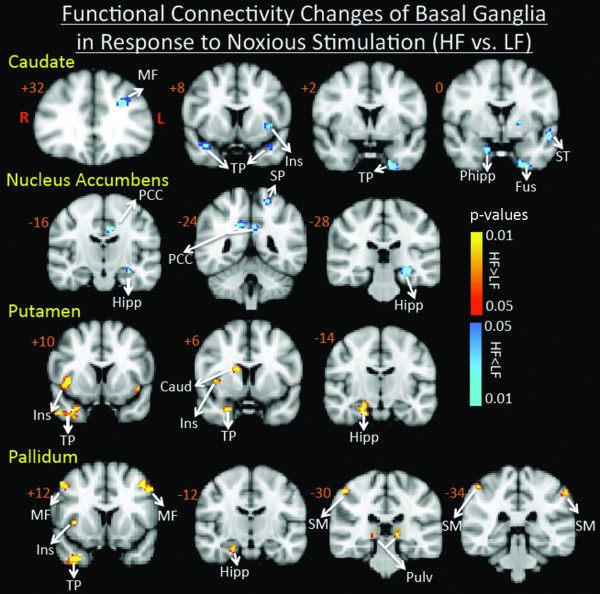
Results: In comparison to LF patients, responses to pain in HF patients were significantly lower in the caudate, putamen and pallidum. Paradoxically, associated with these lower responses in HF patients, gray matter volume of the right and left caudate nuclei were significantly larger than in the LF patients. Functional connectivity analysis revealed additional differences between the two groups in regard to response to pain.
Conclusions: Supported by current understanding of basal ganglia role in pain processing, the findings suggest a significant role of the basal ganglia in the pathophysiology of the episodic migraine.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
