

Feasibility and acceptability of using bronchial hyperresponsiveness to manage asthma in primary care: a pilot study
- PMID: 21938353
- PMCID: PMC6547886
- DOI: 10.4104/pcrj.2011.00079
Feasibility and acceptability of using bronchial hyperresponsiveness to manage asthma in primary care: a pilot study
Abstract
Aims: To determine if indirect testing for bronchial hyperresponsiveness (BHR) to monitor inhaled corticosteroid (ICS) treatment in asthma is feasible and acceptable in primary care.
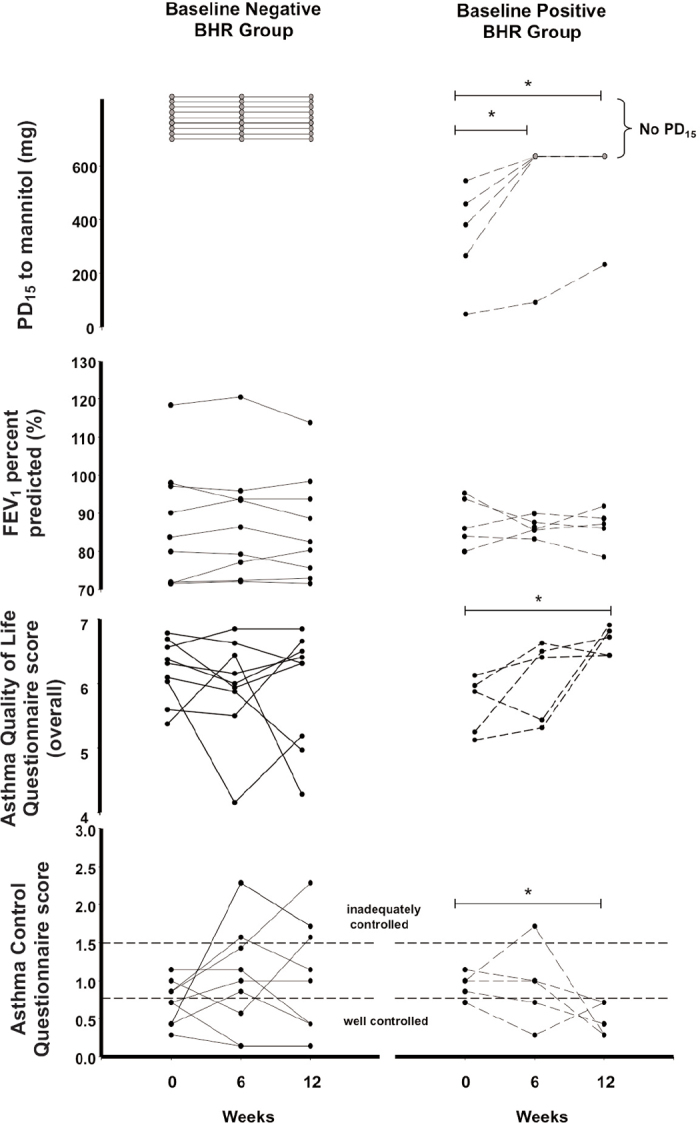
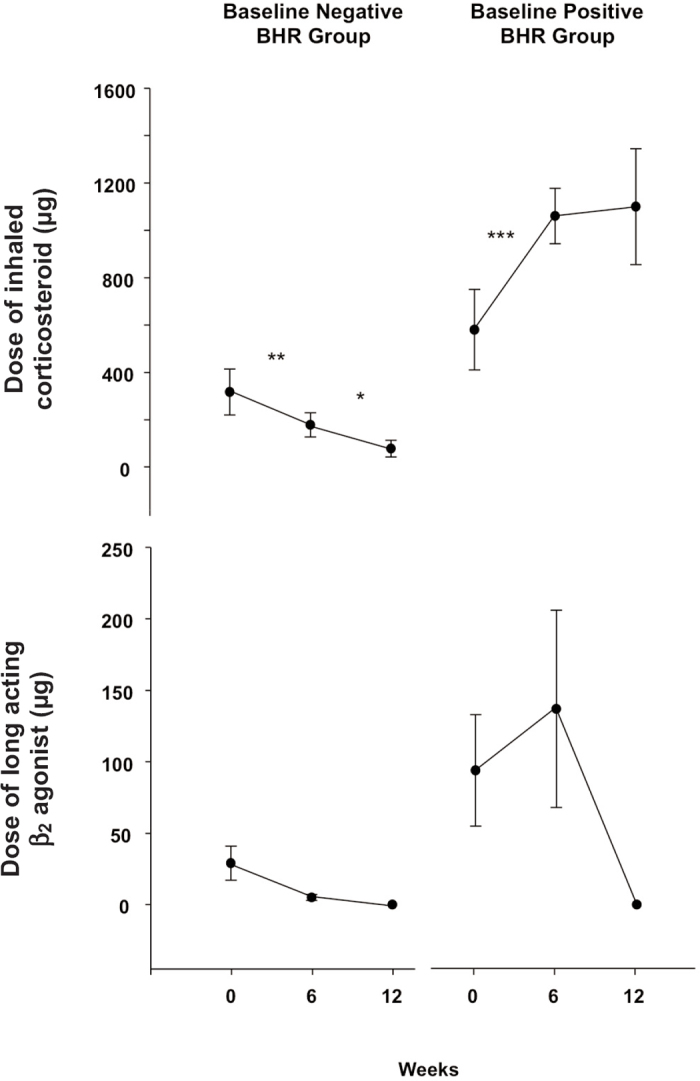
Methods: Fourteen adult patients with asthma aged 22-70 years (4M:10F, forced expiratory volume in 1 s >70% predicted) taking ICS performed a test for BHR using mannitol on three visits 6 weeks apart. ICS dose adjustments were made based on the presence of BHR. The Asthma Quality of Life Questionnaire (AQLQ) and the Asthma Control Questionnaire were used at each visit. A semi structured interview at study exit assessed subject acceptability.
Results: BHR did not return in those with no BHR at study entry (n=9) with decreasing ICS dose. Improvements in BHR with increasing ICS dose (n=5) were observed with clinically significant improvements in AQLQ (mean score increase >0.5, p=0.02). Feasibility and acceptability of BHR testing was demonstrated.
Conclusions: It is feasible and acceptable to perform BHR testing using mannitol to help identify patients with asthma who would benefit from ICS dose increases and those with no BHR who could have a dose reduction.
Trial registration: Australia New Zealand Clinical Trial Registry ACTRN12610000807055.
Conflict of interest statement
JAT holds shares in Pharmaxis Ltd. NJG has no conflict of interest. JDB receives royalties from the sale of Aridol™/Osmohale™, holds shares in Pharmaxis Ltd, and has acted as a consultant to Pharmaxis Ltd.
Figures
Comment in
-
Asthma monitoring in primary care: time to gather more robust evidence.Prim Care Respir J. 2012 Mar;21(1):4-5. doi: 10.4104/pcrj.2012.00005. Prim Care Respir J. 2012. PMID: 22273630 Free PMC article. No abstract available.
References
-
- Rosi E, Ronchi MC, Grazzini M, Duranti R, Scano G. Sputum analysis, bronchial hyperresponsiveness, and airway function in asthma: results of a factor analysis. J Allergy Clin Immunol 1999;103(2 Pt 1):232–7. http://dx.doi.org/10.1016/S0091-6749(99)70496-3 - PubMed
-
- Sont JK, Han J, van Krieken JM, et al. Relationship between the inflammatory infiltrate in bronchial biopsy specimens and clinical severity of asthma in patients treated with inhaled steroids. Thorax 1996;51(5):496–502. http://dx.doi.org/10.1136/thx.51.5.496 - PMC - PubMed
-
- Chapman KR, Boulet LP, Rea RM, Franssen E. Suboptimal asthma control: prevalence, detection and consequences in general practice. Eur Respir J 2008;31(2):320–5. http://dx.doi.org/10.1183/09031936.00039707 - PubMed
-
- Rabe KF, Adachi M, Lai CK, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J Allergy Clin Immunol 2004;114(1):40–7. http://dx.doi.org/10.1016/j.jaci.2004.04.042 - PubMed
-
- Horne R, Price D, Cleland J, et al. Can asthma control be improved by understanding the patient's perspective? BMC Pulm Med 2007;7:8. http://dx.doi.org/10.1186/1471-2466-7-8 - PMC - PubMed