

Charged-particle therapy for hepatocellular carcinoma
- PMID: 21939857
- PMCID: PMC3230301
- DOI: 10.1016/j.semradonc.2011.05.007
Charged-particle therapy for hepatocellular carcinoma
Abstract
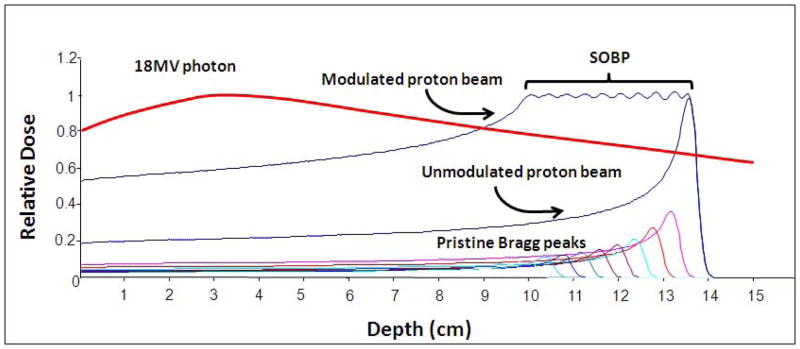
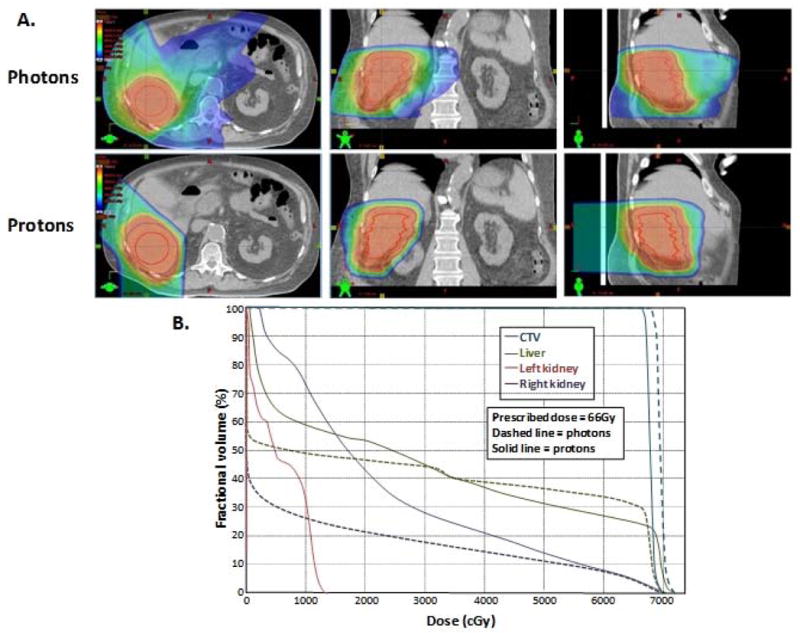
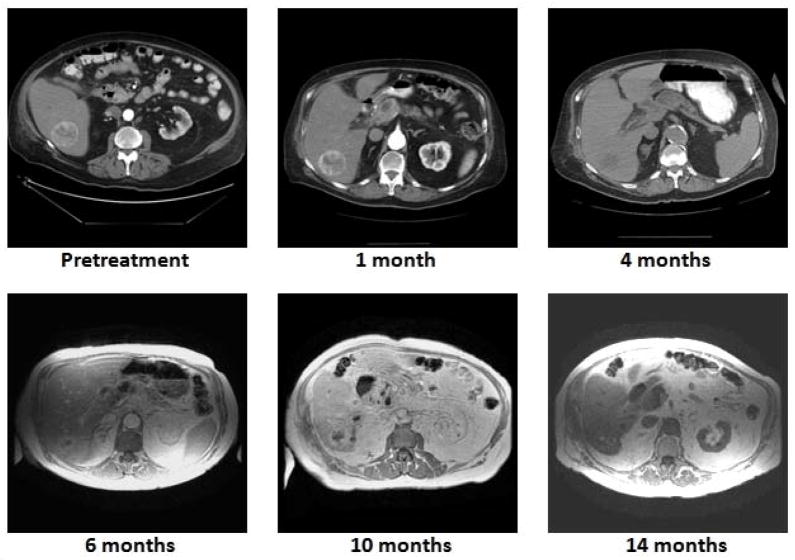
Historically, the use of external-beam radiotherapy for hepatocellular carcinoma (HCC) has been limited by toxicity to the uninvolved liver and surrounding structures. Advances in photon radiotherapy have improved dose conformality to the tumor and facilitated dose escalation, a key contributor to improved HCC radiation treatment outcomes. However, despite these advances in photon radiotherapy, significant volumes of liver still receive low doses of radiation that can preclude dose escalation, particularly in patients with limited functional liver reserves. By capitalizing on the lack of exit dose along the beam path beyond the tumor and higher biological effectiveness, charged-particle therapy offers the promise of maximizing tumor control via dose escalation without excessive liver toxicity. In this review, we discuss the distinctive biophysical attributes of both proton and carbon ion radiotherapy, particularly as they pertain to treatment of HCC. We also review the available literature regarding clinical outcomes and the toxicity of using charged particles for the treatment of HCC.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127:S5–S16. - PubMed
-
- Dawson LA, McGinn CJ, Normolle D, Ten Haken RK, Walker S, Ensminger W, Lawrence TS. Escalated focal liver radiation and concurrent hepatic artery fluorodeoxyuridine for unresectable intrahepatic malignancies. J Clin Oncol. 2000;18:2210–2218. - PubMed
-
- Seong J, Park HC, Han KH, Chon CY. Clinical results and prognostic factors in radiotherapy for unresectable hepatocellular carcinoma: a retrospective study of 158 patients. Int J Radiat Oncol Biol Phys. 2003;55:329–336. - PubMed
-
- Park HC, Seong J, Han KH, Chon CY, Moon YM, Suh CO. Dose-response relationship in local radiotherapy for hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2002;54:150–155. - PubMed
-
- Wang X, Krishnan S, Zhang X, Dong L, Briere T, Crane CH, Martel M, Gillin M, Mohan R, Beddar S. Proton radiotherapy for liver tumors: dosimetric advantages over photon plans. Med Dosim. 2008;33:259–267. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
