

Management of refractory status epilepticus in adults: still more questions than answers
- PMID: 21939901
- PMCID: PMC3202016
- DOI: 10.1016/S1474-4422(11)70187-9
Management of refractory status epilepticus in adults: still more questions than answers
Abstract
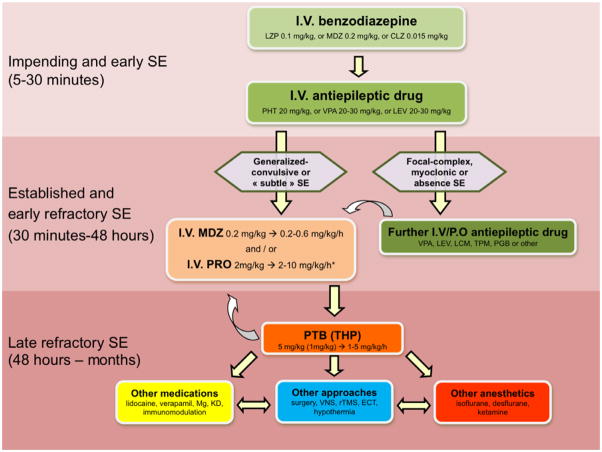
Refractory status epilepticus (RSE) is defined as status epilepticus that continues despite treatment with benzodiazepines and one antiepileptic drug. RSE should be treated promptly to prevent morbidity and mortality; however, scarce evidence is available to support the choice of specific treatments. Major independent outcome predictors are age (not modifiable) and cause (which should be actively targeted). Recent recommendations for adults suggest that the aggressiveness of treatment for RSE should be tailored to the clinical situation. To minimise intensive care unit-related complications, focal RSE without impairment of consciousness might initially be approached conservatively; conversely, early induction of pharmacological coma is advisable in generalised convulsive forms of the disorder. At this stage, midazolam, propofol, or barbiturates are the most commonly used drugs. Several other treatments, such as additional anaesthetics, other antiepileptic or immunomodulatory compounds, or non-pharmacological approaches (eg, electroconvulsive treatment or hypothermia), have been used in protracted RSE. Treatment lasting weeks or months can sometimes result in a good outcome, as in selected patients after encephalitis or autoimmune disorders. Well designed prospective studies of RSE are urgently needed.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Coeytaux A, Jallon P, Galobardes B, Morabia A. Incidence of status epilepticus in French-speaking Switzerland: (EPISTAR) Neurology. 2000;55(5):693–7. - PubMed
-
- DeLorenzo RJ, Hauser WA, Towne AR, Boggs JG, Pellock JM, Penberthy L, et al. A prospective, population-based epidemiologic study of status epilepticus in Richmond, Virginia. Neurology. 1996;46(4):1029–35. - PubMed
-
- Knake S, Rosenow F, Vescovi M, Oertel WH, Mueller HH, Wirbatz A, et al. Incidence of status epilepticus in adults in Germany: a prospective, population-based study. Epilepsia. 2001;42(6):714–8. - PubMed
-
- Lowenstein DH, Alldredge BK. Status epilepticus. N Engl J Med. 1998;338(14):970–6. - PubMed
-
- Holtkamp M. Treatment strategies for refractory status epilepticus. Curr Opin Crit Care. 2011;17(2):94–100. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
