

Association between type of health insurance and elective cesarean deliveries: New Jersey, 2004-2007
- PMID: 21940911
- PMCID: PMC3222406
- DOI: 10.2105/AJPH.2011.300333
Association between type of health insurance and elective cesarean deliveries: New Jersey, 2004-2007
Abstract
Objectives: I examined the relationship between insurance coverage, which may influence physician incentives and maternal choices, and cesarean delivery before labor.
Methods: I analyzed hospital discharge data for mothers without previous cesarean deliveries in New Jersey between 2004 and 2007, with adjustment for maternal age, race, marital status, and maternal, fetal, and placental conditions.
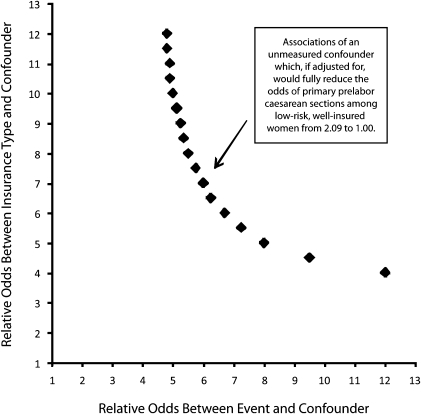
Results: Nearly 1 in 7 women (13.9%) had a cesarean delivery without laboring. Insurance status was strongly associated with cesarean birth. Women insured by Medicaid (adjusted relative risk [ARR] = 0.88; 95% confidence interval [CI] = 0.84, 0.91) or self-paying (ARR = 0.81; 95% CI = 0.78, 0.85) had a significantly lower likelihood, and women insured by BlueCross (ARR = 1.06; 95% CI = 1.03, 1.09) or standard commercial plans (ARR = 1.06; 95% CI = 1.02, 1.10) had a significantly higher likelihood of cesarean delivery than did women insured by commercial health maintenance organizations. These associations persisted in subsets restricted to lower-risk women and in qualitative sensitivity analyses for a hypothetical single, binary, unmeasured confounder.
Conclusions: Insurance status has a small, independent impact on whether a woman without a previous cesarean delivery proceeds to labor or has a cesarean delivery without labor.
Figures
Similar articles
-
Does medical insurance type (private vs public) influence the physician's decision to perform Caesarean delivery?J Med Ethics. 2012 Aug;38(8):470-3. doi: 10.1136/medethics-2011-100209. Epub 2012 May 5. J Med Ethics. 2012. PMID: 22562949
-
Surgical site infection risk following cesarean deliveries covered by Medicaid or private insurance.Infect Control Hosp Epidemiol. 2019 Jun;40(6):639-648. doi: 10.1017/ice.2019.66. Epub 2019 Apr 9. Infect Control Hosp Epidemiol. 2019. PMID: 30963987
-
Prevalence, Disparities, And Determinants Of Primary Cesarean Births Among First-Time Mothers In Mexico.Health Aff (Millwood). 2017 Apr 1;36(4):714-722. doi: 10.1377/hlthaff.2016.1084. Health Aff (Millwood). 2017. PMID: 28373338
-
Health insurance coverage, neonatal mortality and caesarean section deliveries: an analysis of vital registration data in Colombia.J Epidemiol Community Health. 2017 May;71(5):505-512. doi: 10.1136/jech-2016-207499. Epub 2016 Sep 26. J Epidemiol Community Health. 2017. PMID: 27669713 Review.
-
Elective cesarean delivery at 38 and 39 weeks: neonatal and maternal risks.Curr Opin Obstet Gynecol. 2015 Apr;27(2):121-7. doi: 10.1097/GCO.0000000000000158. Curr Opin Obstet Gynecol. 2015. PMID: 25689238 Review.
Cited by
-
Women's experience of agency and respect in maternity care by type of insurance in California.PLoS One. 2020 Jul 27;15(7):e0235262. doi: 10.1371/journal.pone.0235262. eCollection 2020. PLoS One. 2020. PMID: 32716927 Free PMC article.
-
Preventing the preventable: Assessing the burden of incessant caesarean deliveries in select Indian states using NFHS-5.PLoS One. 2025 Apr 23;20(4):e0320041. doi: 10.1371/journal.pone.0320041. eCollection 2025. PLoS One. 2025. PMID: 40267119 Free PMC article.
-
Health system factors and caesarean sections in Kosovo: a cross-sectional study.BMJ Open. 2019 Apr 11;9(4):e026702. doi: 10.1136/bmjopen-2018-026702. BMJ Open. 2019. PMID: 30975683 Free PMC article.
-
Factors associated with increased cesarean risk among African American women: evidence from California, 2010.Am J Public Health. 2015 May;105(5):956-62. doi: 10.2105/AJPH.2014.302381. Epub 2015 Mar 19. Am J Public Health. 2015. PMID: 25790391 Free PMC article.
-
Trends in Hispanic and non-Hispanic white cesarean delivery rates on the US-Mexico border, 2000-2015.PLoS One. 2018 Sep 5;13(9):e0203550. doi: 10.1371/journal.pone.0203550. eCollection 2018. PLoS One. 2018. PMID: 30183758 Free PMC article.
References
-
- Appropriate technology for birth. Lancet. 1985;2(8452):436–437 - PubMed
-
- National Institutes of Health state-of-the-science conference statement: cesarean delivery on maternal request March 27–29, 2006. Obstet Gynecol. 2006;107(6):1386–1397 - PubMed
-
- Kringeland T, Daltveit AK, Moller A. What characterizes women in Norway who wish to have a caesarean section? Scand J Public Health. 2009;37(4):364–371 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
