

Is Drotrecogin alfa (activated) for adults with severe sepsis, cost-effective in routine clinical practice?
- PMID: 21943177
- PMCID: PMC3334774
- DOI: 10.1186/cc10468
Is Drotrecogin alfa (activated) for adults with severe sepsis, cost-effective in routine clinical practice?
Abstract
Introduction: Previous cost-effectiveness analyses (CEA) reported that Drotrecogin alfa (DrotAA) is cost-effective based on a Phase III clinical trial (PROWESS). There is little evidence on whether DrotAA is cost-effective in routine clinical practice. We assessed whether DrotAA is cost-effective in routine practice for adult patients with severe sepsis and multiple organ systems failing.
Methods: This CEA used data from a prospective cohort study that compared DrotAA versus no DrotAA (control) for severe sepsis patients with multiple organ systems failing admitted to critical care units in England, Wales, and Northern Ireland. The cohort study used case-mix and mortality data from a national audit, linked with a separate audit of DrotAA infusions. Re-admissions to critical care and corresponding mortality were recorded for four years. Patients receiving DrotAA (n = 1,076) were matched to controls (n = 1,650) with a propensity score (Pscore), and Genetic Matching (GenMatch). The CEA projected long-term survival to report lifetime incremental costs per quality-adjusted life year (QALY) overall, and for subgroups with two or three to five organ systems failing at baseline.
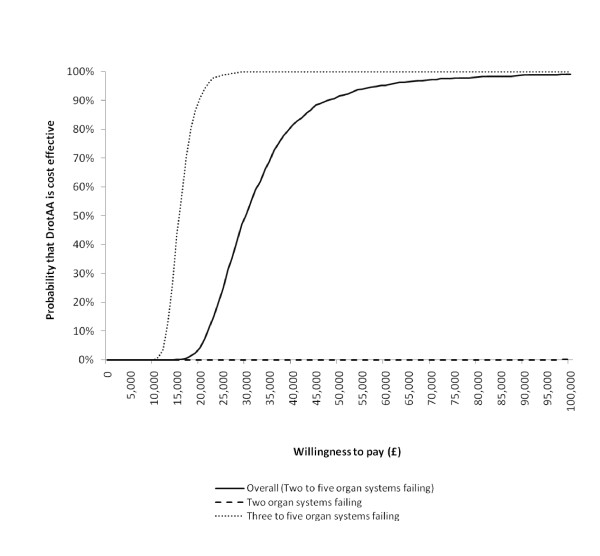
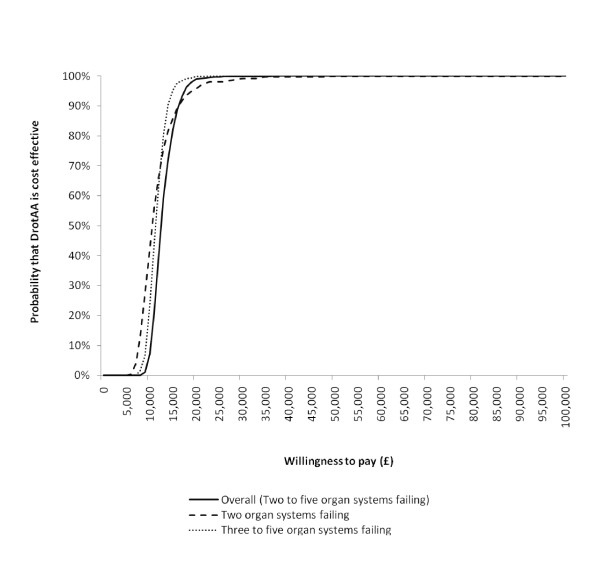
Results: The incremental costs per QALY for DrotAA were £30,000 overall, and £16,000 for the subgroups with three to five organ systems failing. For patients with two organ systems failing, DrotAA resulted in an average loss of one QALY at an incremental cost of £15,000. When the subgroup with two organ systems was restricted to patients receiving DrotAA within 24 hours, DrotAA led to a gain of 1.2 QALYs at a cost per QALY of £11,000. The results were robust to other assumptions including the approach taken to projecting long-term outcomes.
Conclusions: DrotAA is cost-effective in routine practice for severe sepsis patients with three to five organ systems failing. For patients with two organ systems failing, this study could not provide unequivocal evidence on the cost-effectiveness of DrotAA.
Figures
References
-
- Brun-Buisson C, Doyon F, Carlet J, Dellamonica P, Gouin F, Lepoutre A, Mercier JC, Offenstadt G, Regnier B. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA. 1995;274:968–974. doi: 10.1001/jama.274.12.968. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
