

Decisions to operate: the ASA grade 5 dilemma
- PMID: 21943459
- PMCID: PMC3365453
- DOI: 10.1308/003588411X581367
Decisions to operate: the ASA grade 5 dilemma
Abstract
Introduction: Deciding to operate on high risk patients suffering catastrophic surgical emergencies can be problematic. Patients are frequently classed as American Society of Anesthesiologists (ASA) grade 5 and, as a result, aggressive but potentially lifesaving intervention is withheld. The aim of our study was to review the short-term outcomes in patients who were classed as ASA grade 5 but subsequently underwent surgery despite this and to compare the ASA scoring model to other predictors of surgical outcome.
Methods: All patients undergoing emergency surgery with an ASA grade of 5 were identified. Patient demographics, indications for surgery, intraoperative findings and outcomes were recorded. In addition to the ASA scores, retrospective Portsmouth Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (P POSSUM) and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were calculated and compared to the observed outcomes.
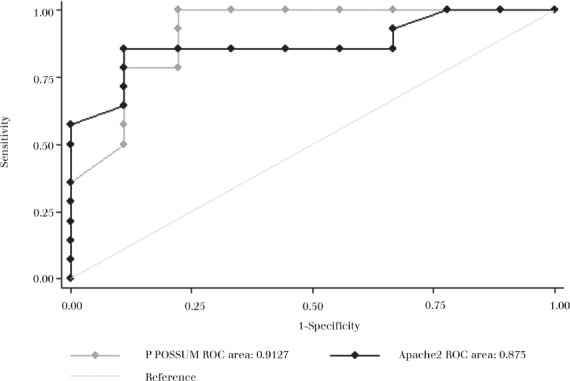
Results: Nine patients (39%) survived to discharge. ASA grade was a poor predictor of outcome. P POSSUM and APACHE II scores correlated significantly with each other and with observed outcomes when predicting surgical mortality. The median stay for survivors in the intensive care unit was nine days.
Conclusions: In times of an ageing population, the number of patients suffering catastrophic surgical events will increase. Intervention, with little hope of a cure, a return to independent living or an acceptable quality of life, leads to unnecessary end-of-life suffering for patients and their relatives, and consumes sparse resources. The accuracy and reliability of ASA grade 5 as an outcome predictor has been questioned. P POSSUM and APACHE II scoring systems are significantly better predictors of outcome and should be used more frequently to aid surgical decision-making in high risk patients.
Figures
References
-
- Williams JH, Collin J. Surgical care of patients over eighty: a predictable crisis at hand. Br J Surg. 1988;75:371–373. - PubMed
-
- Rørbaek-Madsen M, Dupont G, Kristensen K, et al. General surgery in patients aged 80 years and older. Br J Surg. 1992;79:1216–1218. - PubMed
-
- Whiteley MS, Prytherch DR, Higgins B, Weaver PC, Prout WG. An evaluation of the POSSUM surgical scoring system. Br J Surg. 1996;83:812–815. - PubMed
-
- Knaus WA, Zimmerman JE, Wagner DP, et al. APACHE – acute physiology and chronic health evaluation: a physiologically based classification system. Crit Care Med. 1981;9:591–597. - PubMed
-
- Saklad M. Grading of patients for surgical procedures. Anesthesiology. 1941;2:281–284.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources