

Gonadotropin-releasing hormone blockers and cardiovascular disease risk: analysis of prospective clinical trials of degarelix
- PMID: 21944083
- PMCID: PMC3712275
- DOI: 10.1016/j.juro.2011.07.035
Gonadotropin-releasing hormone blockers and cardiovascular disease risk: analysis of prospective clinical trials of degarelix
Abstract
Purpose: We investigated associations of baseline cardiovascular disease risk profile, dosing regimen and treatment duration with incident cardiovascular disease events during androgen deprivation therapy with degarelix in patients with prostate cancer.
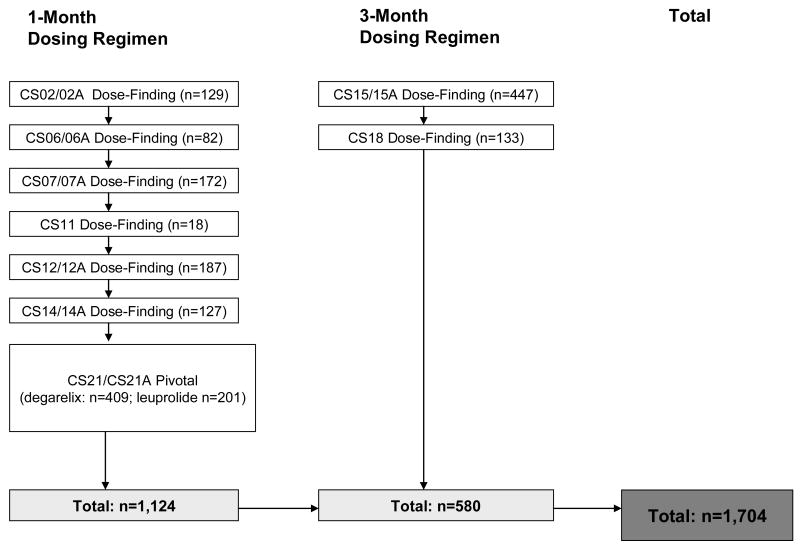
Materials and methods: Data on 1,704 men who participated in a total of 9 clinical trials were pooled for analysis. Patients received treatment with 1-month (20 to 240 mg) or 3-month (240 to 480 mg) doses of degarelix for an average of 22 months. End points were ischemic heart disease, cerebrovascular disorders, arterial thrombotic/embolic events and intermittent claudication.
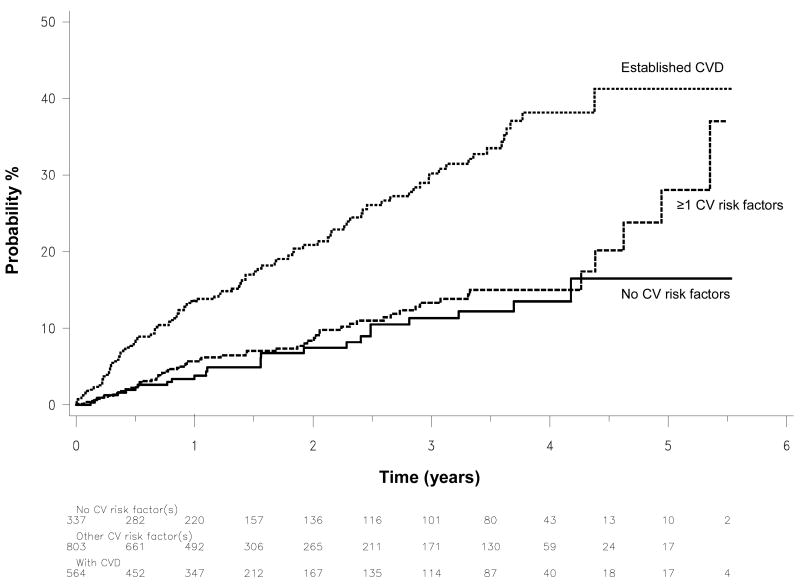
Results: First time cardiovascular disease events were reported in 92 men in the year before study entry and in 168 after degarelix treatment. Event rates were similar before and after degarelix treatment in the total population (5.5 vs 6.1/100 person-years, p = 0.45) and in men without cardiovascular disease (5.6 vs 4.3/100 person-years, p = 0.11). In contrast, event rates appeared higher after degarelix treatment in men with cardiovascular disease at baseline (5.3 to 10.5 events per 100 person-years, p = 0.0013). On multivariate analysis cardiovascular disease at baseline was the strongest independent predictor of events, followed by older age, alcohol abstinence and obesity (each p <0.05). Degarelix dose and schedule were not independently associated with cardiovascular disease events.
Conclusions: In men with prostate cancer observed rates of cardiovascular disease events were similar before and after degarelix treatment. Events were largely confined to men with preexisting cardiovascular disease and further modulated by age and modifiable risk factors. Randomized, controlled trials and longer followup are key to fully clarify the comparative safety of gonadotropin-releasing hormone antagonists vs agonists.
Copyright © 2011 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Van Poppel H, Nilsson S. Testosterone surge: rationale for gonadotropin-releasing hormone blockers? Urology. 2008;71:1001–6. - PubMed
-
- Cookson MS, Sarosdy MF. Hormonal therapy for metastatic prostate cancer: issues of timing and total androgen ablation. South Med J. 1994;87:1–6. - PubMed
-
- Levine GN, D'Amico AV, Berger P, et al. American Heart Association Council on Clinical Cardiology and Council on Epidemiology and Prevention, the American Cancer Society, and the American Urological Association Androgen-Deprivation Therapy in Prostate Cancer and Cardiovascular Risk. Circulation. 2010;121:833–840. - PMC - PubMed
-
- Keating NL, O'Malley AJ, Smith MR. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J Clin Oncol. 2006;24:4448–4456. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
