

Retroperitoneal tumours: review of management
- PMID: 21944791
- PMCID: PMC3363075
- DOI: 10.1308/003588411X571944
Retroperitoneal tumours: review of management
Abstract
Introduction: The retroperitoneum can host a wide spectrum of pathologies, including a variety of rare benign tumours and malignant neoplasms that can be either primary or metastatic lesions. Retroperitoneal tumours can cause a diagnostic dilemma and present several therapeutic challenges because of their rarity, relative late presentation and anatomical location, often in close relationship with several vital structures in the retroperitoneal space.
Materials and methods: A comprehensive literature search was conducted using PubMed. Relevant international articles published in the last ten years were assessed. The keywords for search purposes included: retroperitoneum, benign, sarcoma, neoplasm, diagnosis and surgery, radiotherapy, chemotherapy. The search was limited to articles published in English. All articles were read in full by the authors and selected for inclusion based on relevance to this article.
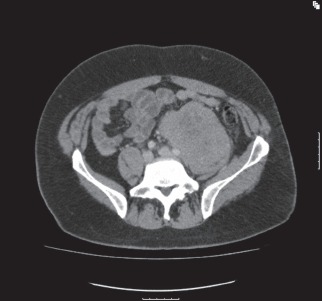
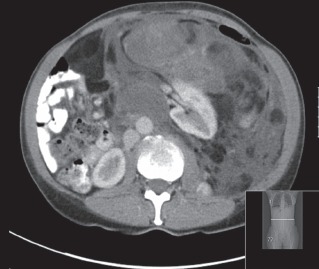
Results: Tumours usually present late and cause symptoms or become palpable once they have reached a significant size. Retroperitoneal tumours are best evaluated with good quality cross-sectional imaging and preoperative histology by core needle biopsy is required when imaging is non-diagnostic. Sarcomas comprise a third of retroperitoneal tumours. Other retroperitoneal neoplasms include lymphomas and epithelial tumours or might represent metastatic disease from known or unknown primary sites. The most common benign pathologies encountered in the retroperitoneum include benign neurogenic tumours, paragangliomas, fibromatosis, renal angiomyolipomas and benign retroperitoneal lipomas.
Conclusions: Complete surgical resection is the only potential curative treatment modality for retroperitoneal sarcomas and is best performed in high-volume centres by a multidisciplinary sarcoma team. The ability completely to resect a retroperitoneal sarcoma and tumour grade remain the most important predictors of local recurrence and disease-specific survival.
Figures







References
-
- National Institute for Health and Clinical Excellence. Improving Outcomes for People with Sarcoma: The Manual. London: NICE; 2006.
-
- Weiss SW, Goldblum JR. Enzinger and Weiss's Soft Tissue Tumors. 4th edn. St Louis, Missouri, US: Mosby; 2001.
-
- Strauss DC, Hayes AJ, Thway K, et al. Surgical management of primary retroperitoneal sarcoma. Br J Surg. 2010;97:698–706. - PubMed
-
- Raut CP, Swallow CJ. Are radical compartmental resections for retroperitoneal sarcomas justified? Ann Surg Oncol. 2010;17:1,481–1,484. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical