

An optimal body mass index range associated with improved immune reconstitution among HIV-infected adults initiating antiretroviral therapy
- PMID: 21946189
- PMCID: PMC3189168
- DOI: 10.1093/cid/cir606
An optimal body mass index range associated with improved immune reconstitution among HIV-infected adults initiating antiretroviral therapy
Abstract
Background: Higher body mass index (BMI) was associated with slower human immunodeficiency virus (HIV) disease progression before the availability of effective antiretroviral therapy (ART), but the relationship between pretreatment BMI and CD4(+) lymphocyte recovery on ART is not well described.
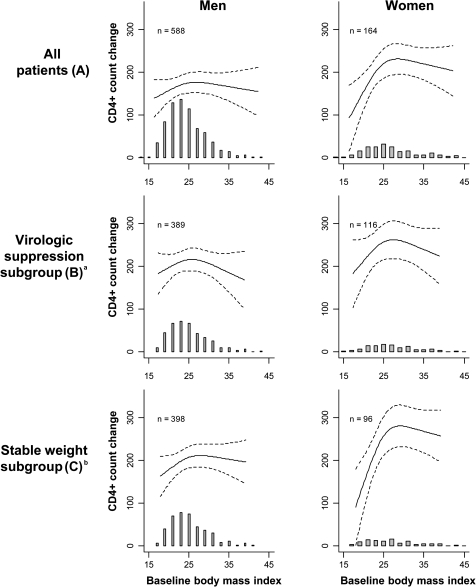
Methods: We conducted an observational cohort study of HIV-infected, ART-naive adults starting treatment at a clinic affiliated with Vanderbilt University in Nashville, Tennessee. We assessed the relationship between pretreatment BMI and CD4(+) lymphocyte count change from baseline to 12 months in all subjects, among those with plasma HIV-1 RNA levels <400 copies/mL for ≥ 6 months and those with <10% change in weight during follow-up. Linear regression models were adjusted for age, sex, race, protease inhibitor usage, year of ART initiation, and baseline CD4(+) lymphocyte count and HIV-1 RNA level.
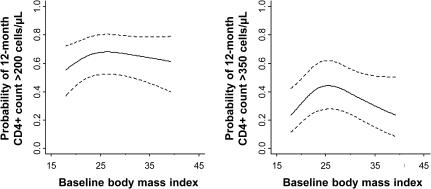
Results: A total of 915 patients met inclusion criteria; 78% were male, and their median age, BMI, and CD4(+) lymphocyte count were 39 years, 24 kg/m², and 171 cells/μL, respectively. The CD4(+) lymphocyte increase at 12 months was greatest among patients with a pretreatment BMI of ~25-30 kg/m² and diminished above and below this range (P = .03). Similar patterns were observed in the subgroup analyses. Among patients with a pretreatment CD4(+) lymphocyte count < 200 cells/μL, a BMI of ~25 kg/m² was associated with the highest odds of reaching a CD4(+) lymphocyte count > 350 cells/μL at 12 months (P = .05).
Conclusions: 12-month immune reconstitution on ART was highest among patients commonly classified as overweight, suggesting there may be an optimal BMI range for immune recovery on ART.
Figures
Similar articles
-
Body mass index and early CD4 T-cell recovery among adults initiating antiretroviral therapy in North America, 1998-2010.HIV Med. 2015 Oct;16(9):572-7. doi: 10.1111/hiv.12259. Epub 2015 May 11. HIV Med. 2015. PMID: 25960080 Free PMC article.
-
Predictive effects of body mass index on immune reconstitution among HIV-infected HAART users in China.BMC Infect Dis. 2019 May 2;19(1):373. doi: 10.1186/s12879-019-3991-6. BMC Infect Dis. 2019. PMID: 31046702 Free PMC article.
-
Short-term and long-term clinical and immunological consequences of stopping antiretroviral therapy in HIV-infected patients with preserved immune function.Antivir Ther. 2013;18(1):125-30. doi: 10.3851/IMP2249. Epub 2012 Jul 18. Antivir Ther. 2013. PMID: 22805174 Clinical Trial.
-
[Consensus document of Gesida and Spanish Secretariat for the National Plan on AIDS (SPNS) regarding combined antiretroviral treatment in adults infected by the human immunodeficiency virus (January 2012)].Enferm Infecc Microbiol Clin. 2012 Jun;30(6):e1-89. doi: 10.1016/j.eimc.2012.03.006. Epub 2012 May 23. Enferm Infecc Microbiol Clin. 2012. PMID: 22633764 Spanish.
-
Pathogenesis and prevention of immune reconstitution disease during antiretroviral therapy.Expert Rev Anti Infect Ther. 2011 Apr;9(4):415-30. doi: 10.1586/eri.11.21. Expert Rev Anti Infect Ther. 2011. PMID: 21504399 Free PMC article. Review.
Cited by
-
Construction and validation of a prognostic nomogram for predicting the survival of HIV/AIDS adults who received antiretroviral therapy: a cohort between 2003 and 2019 in Nanjing.BMC Public Health. 2022 Jan 6;22(1):30. doi: 10.1186/s12889-021-12249-8. BMC Public Health. 2022. PMID: 34991536 Free PMC article.
-
Nutrition indicators as potential predictors of AIDS-defining illnesses among ARV-naïve HIV-positive adults in Kapiri Mposhi, Zambia 2008-2009.PLoS One. 2019 Jul 2;14(7):e0219111. doi: 10.1371/journal.pone.0219111. eCollection 2019. PLoS One. 2019. PMID: 31265479 Free PMC article.
-
Changes in T-lymphocyte subsets and risk factors in human immunodeficiency virus-negative patients with active tuberculosis.Infection. 2020 Aug;48(4):585-595. doi: 10.1007/s15010-020-01451-2. Epub 2020 May 29. Infection. 2020. PMID: 32472529 Free PMC article.
-
Circulating immunoglobulins and transient lymphocytopenia in a sub-study of CAPRISA 012B, testing HIV monoclonal antibodies in a phase 1 trial.Sci Rep. 2024 Jun 12;14(1):13499. doi: 10.1038/s41598-024-63902-2. Sci Rep. 2024. PMID: 38866888 Free PMC article. Clinical Trial.
-
High baseline body mass index predicts recovery of CD4+ T lymphocytes for HIV/AIDS patients receiving long-term antiviral therapy.PLoS One. 2022 Dec 30;17(12):e0279731. doi: 10.1371/journal.pone.0279731. eCollection 2022. PLoS One. 2022. PMID: 36584083 Free PMC article.
References
-
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348:1625–38. - PubMed
-
- Flegal KM, Graubard BI, Williamson DF, Gail MH. Cause-specific excess deaths associated with underweight, overweight, and obesity. JAMA. 2007;298:2028–37. - PubMed
-
- Wilson PW, D'Agostino RB, Sullivan L, Parise H, Kannel WB. Overweight and obesity as determinants of cardiovascular risk: the Framingham experience. Arch Intern Med. 2002;162:1867–72. - PubMed
-
- Shor-Posner G, Campa A, Zhang G, et al. When obesity is desirable: a longitudinal study of the Miami HIV-1-infected drug abusers (MIDAS) cohort. J Acquir Immune Defic Syndr. 2000;23:81–8. - PubMed
-
- Shuter J, Chang CJ, Klein RS. Prevalence and predictive value of overweight in an urban HIV care clinic. J Acquir Immune Defic Syndr. 2001;26:291–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
