

Occurrence and impact of delayed cerebral ischemia after coiling and after clipping in the International Subarachnoid Aneurysm Trial (ISAT)
- PMID: 21947244
- PMCID: PMC3319891
- DOI: 10.1007/s00415-011-6243-2
Occurrence and impact of delayed cerebral ischemia after coiling and after clipping in the International Subarachnoid Aneurysm Trial (ISAT)
Abstract
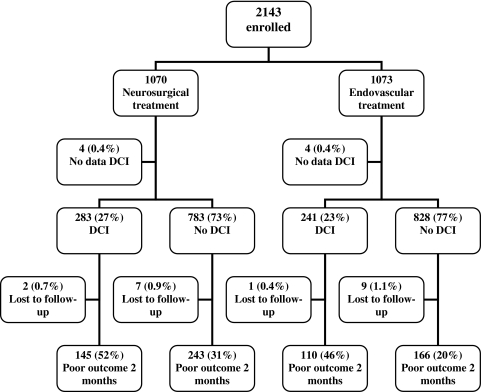
Delayed cerebral ischemia (DCI) is an important cause of poor outcome after aneurysmal subarachnoid hemorrhage (SAH). We studied differences in incidence and impact of DCI as defined clinically after coiling and after clipping in the International Subarachnoid Aneurysm Trial. We calculated odds ratios (OR) for DCI for clipping versus coiling with logistic regression analysis. With coiled patients without DCI as the reference group, we calculated ORs for poor outcome at 2 months and 1 year for coiled patients with DCI and for clipped patients without, and with DCI. With these ORs, we calculated relative excess risk due to Interaction (RERI). Clipping increased the risk of DCI compared to coiling in the 2,143 patients OR 1.24, 95% confidence interval (95% CI 1.01-1.51). Coiled patients with DCI, clipped patients without DCI, and clipped patients with DCI all had higher risks of poor outcome than coiled patients without DCI. Clipping and DCI showed no interaction for poor outcome at 2 months: RERI 0.12 (95% CI -1.16 to 1.40) or 1 year: RERI -0.48 (95% CI -1.69 to 0.74). Only for patients treated within 4 days, coiling and DCI was associated with a poorer outcome at 1 year than clipping and DCI (RERI -2.02, 95% CI -3.97 to -0.08). DCI was more common after clipping than after coiling in SAH patients in ISAT. Impact of DCI on poor outcome did not differ between clipped and coiled patients, except for patients treated within 4 days, in whom DCI resulted more often in poor outcome after coiling than after clipping.
Figures
References
-
- Roos YB, de Haan RJ, Beenen LF, Groen RJ, Albrecht KW, Vermeulen M. Complications and outcome in patients with aneurysmal subarachnoid haemorrhage: a prospective hospital based cohort study in the Netherlands. J Neurol Neurosurg Psychiatry. 2000;68:337–341. doi: 10.1136/jnnp.68.3.337. - DOI - PMC - PubMed
-
- Rivero-Arias O, Wolstenholme J, Gray A, Molyneux AJ, Kerr RS, Yarnold JA, Sneade M. The costs and prognostic characteristics of ischaemic neurological deficit due to subarachnoid haemorrhage in the United Kingdom: evidence from the MRC International Subarachnoid Aneurysm Trial. J Neurol. 2009;79:373–378. - PubMed
-
- Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, Holman R. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2,143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 2002;360:1267–1274. doi: 10.1016/S0140-6736(02)11314-6. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
