

Encounter frequency and serum glucose level, blood pressure, and cholesterol level control in patients with diabetes mellitus
- PMID: 21949161
- PMCID: PMC3692291
- DOI: 10.1001/archinternmed.2011.400
Encounter frequency and serum glucose level, blood pressure, and cholesterol level control in patients with diabetes mellitus
Abstract
Background: More frequent patient-provider encounters may lead to faster control of hemoglobin A1c level, blood pressure (BP), and low-density lipoprotein (LDL) cholesterol (LDL-C) level (hereafter referred to as hemoglobin A1c, BP, and LDL-C) and improve outcomes, but no guidelines exist for how frequently patients with diabetes mellitus (DM) should be seen.
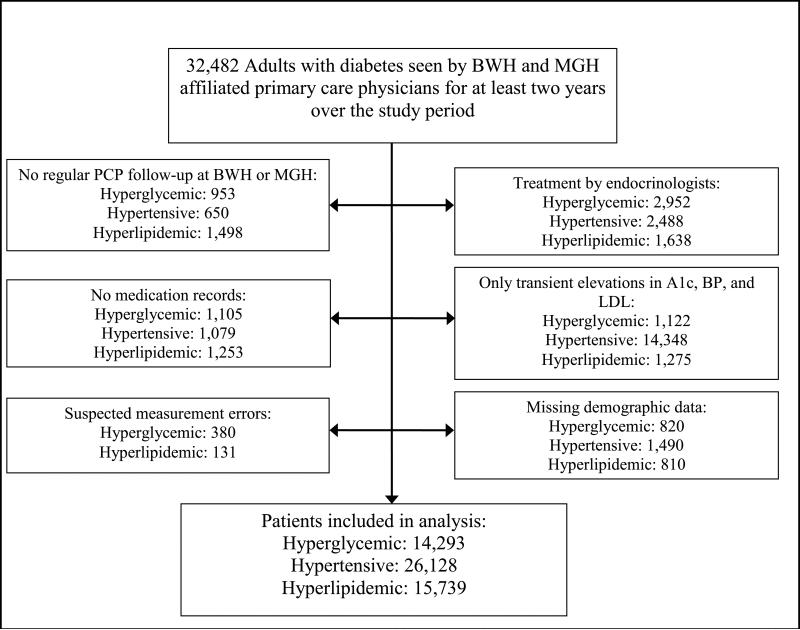
Methods: This retrospective cohort study analyzed 26,496 patients with diabetes and elevated hemoglobin A1c, BP, and/or LDL-C treated by primary care physicians at 2 teaching hospitals between January 1, 2000, and January 1, 2009. The relationship between provider encounter (defined as a note in the medical record) frequency and time to hemoglobin A1c, BP, and LDL-C control was assessed.
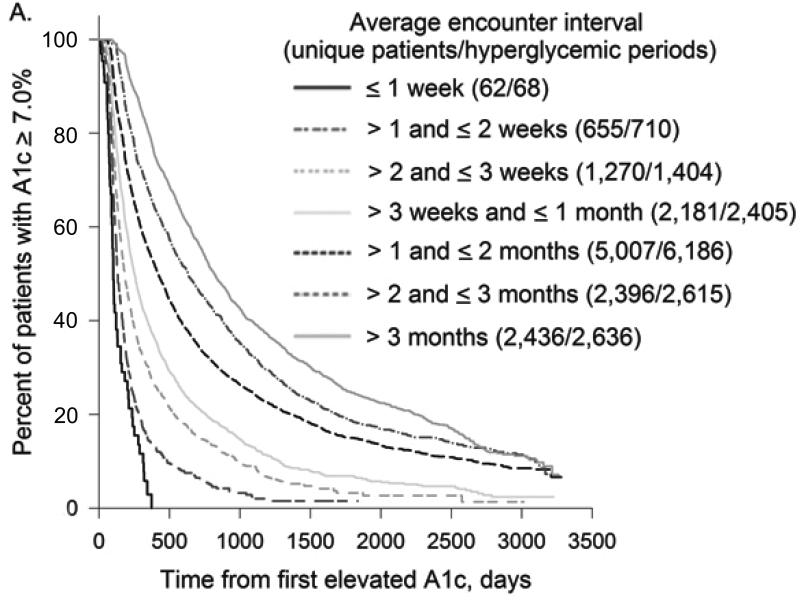
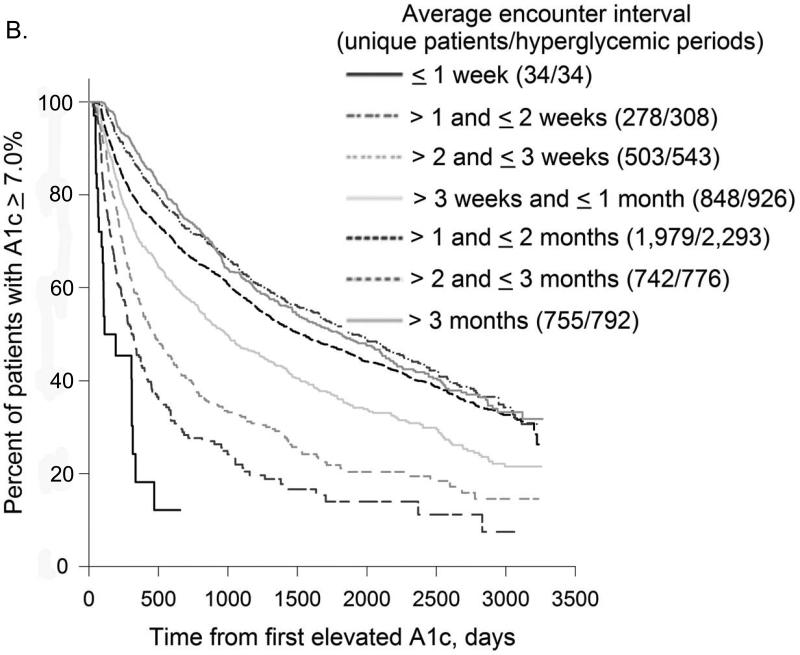
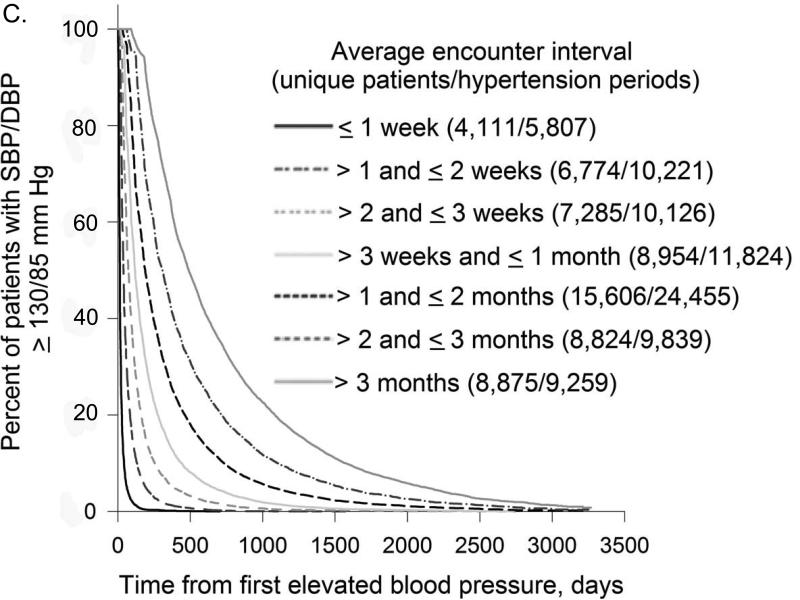
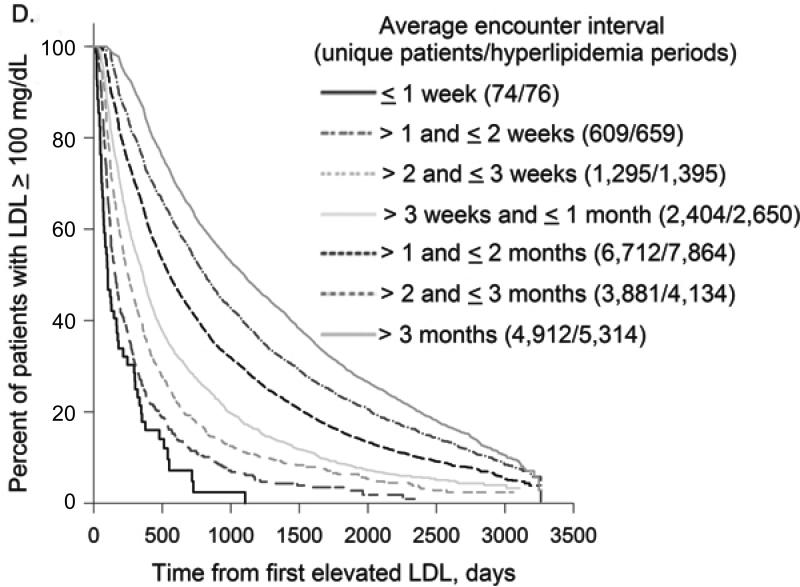
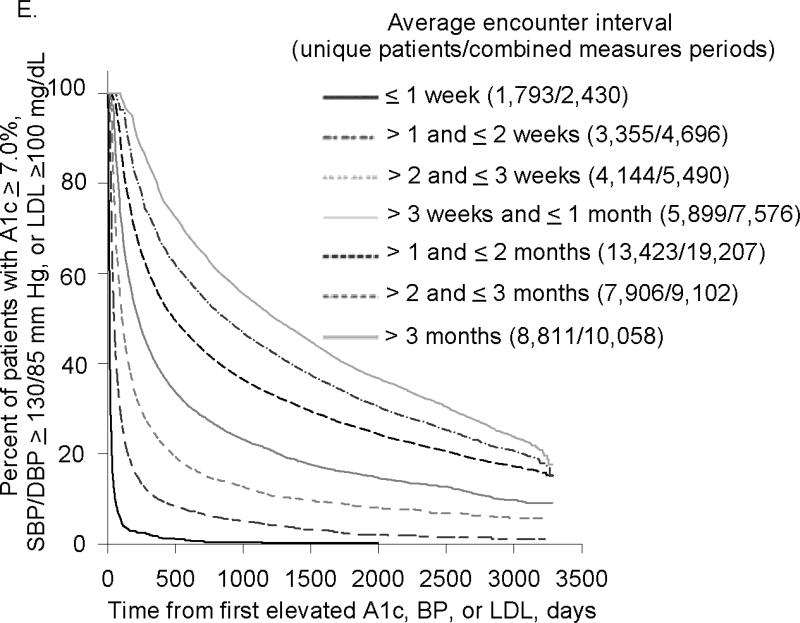
Results: Comparing patients who had encounters with their physicians between 1 to 2 weeks vs 3 to 6 months, median time to hemoglobin A1c less than 7.0% was 4.4 vs 24.9 months (not receiving insulin) and 10.1 vs 52.8 months (receiving insulin); median time to BP lower than 130/85 mm Hg was 1.3 vs 13.9 months; and median time to LDL-C less than 100 mg/dL was 5.1 vs 32.8 months, respectively (P<.001 for all). In multivariable analysis, doubling the time between physician encounters led to an increase in median time to hemoglobin A1c (not receiving [35%] and receiving [17%] insulin), BP (87%), and LDL-C (27%) targets (P<.001 for all). Time to control decreased progressively as encounter frequency increased up to once every 2 weeks for most targets, consistent with the pharmacodynamics of the respective medication classes.
Conclusions: Primary care provider encounters every 2 weeks are associated with fastest achievement of hemoglobin A1c, BP, and LDL-C targets for patients with diabetes mellitus.
Figures
Comment in
-
When it comes to primary care, more may be more: comment on "Encounter frequency and serum glucose level, blood pressure, and cholesterol level control in patients with diabetes mellitus".Arch Intern Med. 2011 Sep 26;171(17):1550-1. doi: 10.1001/archinternmed.2011.403. Arch Intern Med. 2011. PMID: 21949162 No abstract available.
-
Better care for patients with diabetes: e-medicine is the goal.Arch Intern Med. 2012 Feb 27;172(4):373; author reply 374-5. doi: 10.1001/archinternmed.2011.783. Arch Intern Med. 2012. PMID: 22371932 No abstract available.
-
A counterargument to encounter frequency and target achievement: measurement variability.Arch Intern Med. 2012 Feb 27;172(4):374; author reply 374-5. doi: 10.1001/archinternmed.2011.807. Arch Intern Med. 2012. PMID: 22371933 No abstract available.
-
Greater diabetes-care contact frequency is associated with more rapid achievement of care goals but interpretation of finding requires consideration of patient adherence and motivation.Evid Based Med. 2012 Aug;17(4):120-1. doi: 10.1136/ebmed-2011-100415. Epub 2012 Mar 14. Evid Based Med. 2012. PMID: 22419770 No abstract available.
References
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004 May;27(5):1047–1053. - PubMed
-
- The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Engl J Med. 1993 Sep 30;329(14):977–986. - PubMed
-
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998 Sep 12;352(9131):837–853. - PubMed
