

Impact of dyslipidemia on cardiovascular risk stratification of hypertensive patients and association of lipid profile with other cardiovascular risk factors: results from the ICEBERG study
- PMID: 21949610
- PMCID: PMC3172055
- DOI: 10.2147/ibpc.s3809
Impact of dyslipidemia on cardiovascular risk stratification of hypertensive patients and association of lipid profile with other cardiovascular risk factors: results from the ICEBERG study
Abstract
Background: Hypertension, dyslipidemia, and other cardiovascular risk factors are linked epidemiologically, clinically, and metabolically. Intensive/Initial Cardiovascular Examination regarding Blood Pressure levels, Evaluation of Risk Groups (ICEBERG) study focuses on the effect of dyslipidemia on cardiovascular risk evaluation and association of lipid profile with other risk factors.
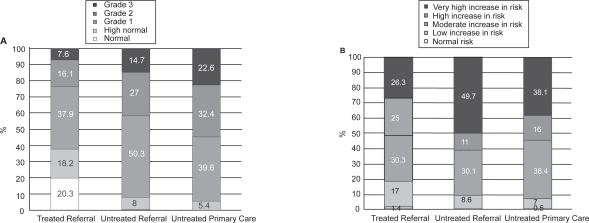
Patients and methods: The ICEBERG study consisted of two sub-protocols: ICEBERG-1, conducted at 20 university hospitals (Referral Group) and ICEBERG-2, conducted at 197 primary healthcare centers (Primary Care Group). Sub-protocol had two patient profiles: patients previously diagnosed with essential hypertension and under medical treatment (Treated Group) and patients with systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg, with no antihypertensive treatment for at least 3 months before inclusion (Untreated Group). Dyslipidemia was evaluated and cardiovascular risk stratification was performed according to ESC/ESH guidelines.
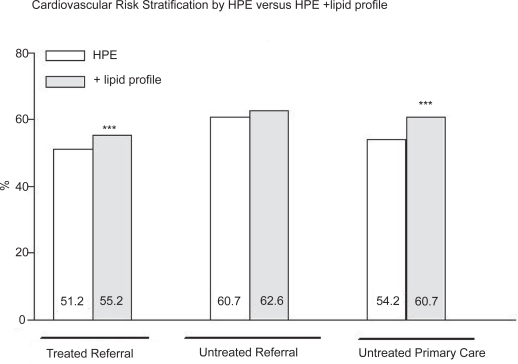
Results: More than half of the treated and untreated subjects were classified into high or very high cardiovascular risk groups. In a total of 1817 patients, the percentage of patients in "high" plus "very high" added risk groups increased to 55.2% in Treated Referral Group (p < 0.001), to 62.6% in Untreated Referral Group (p = 0.25) and to 60.7% in Untreated Primary Care Group (p < 0.001), by re-evaluation of patients' lipid values.
Conclusions: Serum lipid levels are useful in stratifying hypertensive patients into cardiovascular risk groups more accurately, for appropriate antihypertensive treatment.
Keywords: cardiovascular disease; dyslipidemia; hypertension.
Figures
Similar articles
-
The impact of plasma high-sensitivity C-reactive protein levels on cardiovascular risk stratification of hypertensive patients: results of the ICEBERG study.J Clin Hypertens (Greenwich). 2007 Jul;9(7):500-5. doi: 10.1111/j.1524-6175.2007.05738.x. J Clin Hypertens (Greenwich). 2007. PMID: 17617758 Free PMC article. Clinical Trial.
-
Intensive cardiovascular examination regarding blood pressure levels: evaluation of risk groups. ICEBERG study.Blood Press. 2006;15(5):291-301. doi: 10.1080/08037050600996644. Blood Press. 2006. PMID: 17380847
-
Evaluation of the metabolic syndrome in hypertensive patients: results from the ICEBERG Study.J Cardiometab Syndr. 2007 Summer;2(3):168-73. doi: 10.1111/j.1559-4564.2007.06530.x. J Cardiometab Syndr. 2007. PMID: 17786080
-
The 2010 Canadian Hypertension Education Program recommendations for the management of hypertension: part 2 - therapy.Can J Cardiol. 2010 May;26(5):249-58. doi: 10.1016/s0828-282x(10)70379-2. Can J Cardiol. 2010. PMID: 20485689 Free PMC article. Review.
-
The 2009 Canadian Hypertension Education Program recommendations for the management of hypertension: Part 2--therapy.Can J Cardiol. 2009 May;25(5):287-98. doi: 10.1016/s0828-282x(09)70492-1. Can J Cardiol. 2009. PMID: 19417859 Free PMC article. Review.
Cited by
-
Heavy khat (Catha edulis) chewing and dyslipidemia as modifiable hypertensive risk factors among patients in Southwest, Ethiopia: Unmatched case-control study.PLoS One. 2021 Oct 26;16(10):e0259078. doi: 10.1371/journal.pone.0259078. eCollection 2021. PLoS One. 2021. PMID: 34699551 Free PMC article.
-
The Role of Integrated Approach to Yoga Therapy-Based Yoga Module in Improving Cardiovascular Functions and Lipid Profile in Hypertensive Patients: A Randomized Controlled Trial.Int J Yoga. 2022 Sep-Dec;15(3):215-221. doi: 10.4103/ijoy.ijoy_107_22. Epub 2023 Jan 16. Int J Yoga. 2022. PMID: 36949834 Free PMC article.
-
Cardiovascular risk assessment of dyslipidemic middle-aged adults without overt cardiovascular disease over the period of 2009-2016 in Lithuania.Lipids Health Dis. 2018 Oct 11;17(1):233. doi: 10.1186/s12944-018-0883-5. Lipids Health Dis. 2018. PMID: 30305084 Free PMC article.
-
Dyslipidemia Associated with Hypertension Increases the Risks for Coronary Heart Disease: A Case-Control Study in Harapan Kita Hospital, National Cardiovascular Center, Jakarta.J Lipids. 2019 Apr 30;2019:2517013. doi: 10.1155/2019/2517013. eCollection 2019. J Lipids. 2019. PMID: 31183219 Free PMC article.
References
-
- American Heart Association. Heart Disease and Stroke Statistics: 2004 Update. Dallas: American Heart Association; 2003.
-
- Austin MA. Plasma triglyceride and coronary heart disease. Arterioscler Thromb. 1991;11:2–14. - PubMed
-
- Ballantyne CM. Low-density lipoproteins and risk for coronary artery disease. Am J Cardiol. 1998;82:3Q–12Q. - PubMed
-
- Borghi C. Interactions between hypercholesterolemia and hypertension: implications for therapy. Curr Opin Nephrol Hypertens. 2002;11:489–96. - PubMed
-
- Brown BG, Zhao XQ, Bardsley J, et al. Secondary prevention of heart disease amongst patients with lipid abnormalities: practice and trends in the Unites States. J Intern Med. 1997;241:283–94. - PubMed
LinkOut - more resources
Full Text Sources
