

Simulation-based estimates of effectiveness and cost-effectiveness of smoking cessation in patients with chronic obstructive pulmonary disease
- PMID: 21949774
- PMCID: PMC3173494
- DOI: 10.1371/journal.pone.0024870
Simulation-based estimates of effectiveness and cost-effectiveness of smoking cessation in patients with chronic obstructive pulmonary disease
Abstract
Background: The medico-economic impact of smoking cessation considering a smoking patient with chronic obstructive pulmonary disease (COPD) is poorly documented.
Objective: Here, considering a COPD smoking patient, the specific burden of continuous smoking was estimated, as well as the effectiveness and the cost-effectiveness of smoking cessation.
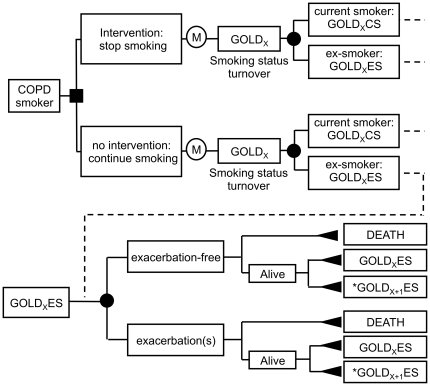
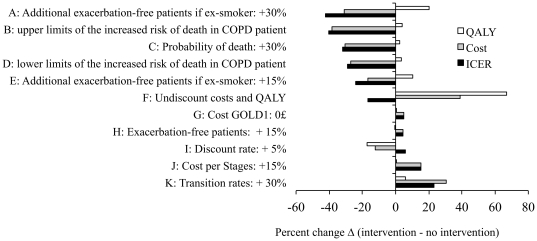
Methods: A multi-state Markov model adopting society's perspective was developed. Simulated cohorts of English COPD patients who are active smokers (all severity stages combined or patients with the same initial severity stage) were compared to identical cohorts of patients who quit smoking at cohort initialization. Life expectancy, quality adjusted life-years (QALY), disease-related costs, and incremental cost-effectiveness ratio (ICER: £/QALY) were estimated, considering smoking cessation programs with various possible scenarios of success rates and costs. Sensitivity analyses included the variation of model key parameters.
Principal findings: At the horizon of a smoking COPD patient's remaining lifetime, smoking cessation at cohort intitialization, relapses being allowed as observed in practice, would result in gains (mean) of 1.27 life-years and 0.68 QALY, and induce savings of -1824 £/patient in the disease-related costs. The corresponding ICER was -2686 £/QALY. Smoking cessation resulted in 0.72, 0.69, 0.64 and 0.42 QALY respectively gained per mild, moderate, severe, and very severe COPD patient, but was nevertheless cost-effective for mild to severe COPD patients in most scenarios, even when hypothesizing expensive smoking cessation intervention programmes associated with low success rates. Considering a ten-year time horizon, the burden of continuous smoking in English COPD patients was estimated to cost a total of 1657 M£ while 452516 QALY would be simultaneously lost.
Conclusions: The study results are a useful support for the setting of smoking cessation programmes specifically targeted to COPD patients.
Conflict of interest statement
Figures
References
-
- Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370:765–773. - PubMed
-
- Scanlon PD, Connett JE, Waller LA, Altose MD, Bailey WC, et al. Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease. The Lung Health Study. Am J Respir Crit Care Med. 2000;161:381–390. - PubMed
-
- Goodman PG, Haw S, Kabir Z, Clancy L. Are there health benefits associated with comprehensive smoke-free laws. Int J Public Health. 2009;54:367–378. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
