

Utility of repeated praziquantel dosing in the treatment of schistosomiasis in high-risk communities in Africa: a systematic review
- PMID: 21949893
- PMCID: PMC3176745
- DOI: 10.1371/journal.pntd.0001321
Utility of repeated praziquantel dosing in the treatment of schistosomiasis in high-risk communities in Africa: a systematic review
Abstract
Background: Controversy persists about the optimal approach to drug-based control of schistosomiasis in high-risk communities. In a systematic review of published studies, we examined evidence for incremental benefits from repeated praziquantel dosing, given 2 to 8 weeks after an initial dose, in Schistosoma-endemic areas of Africa.
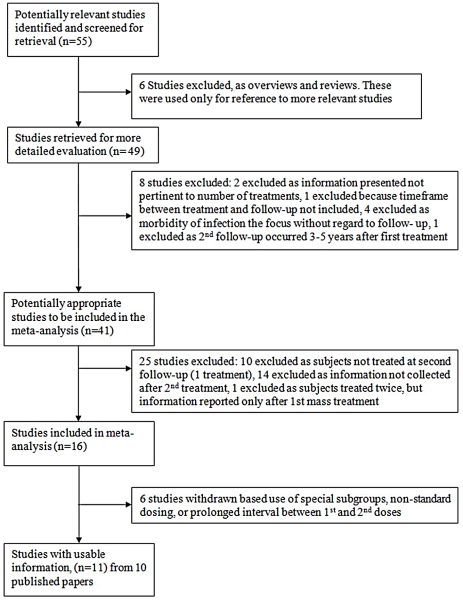
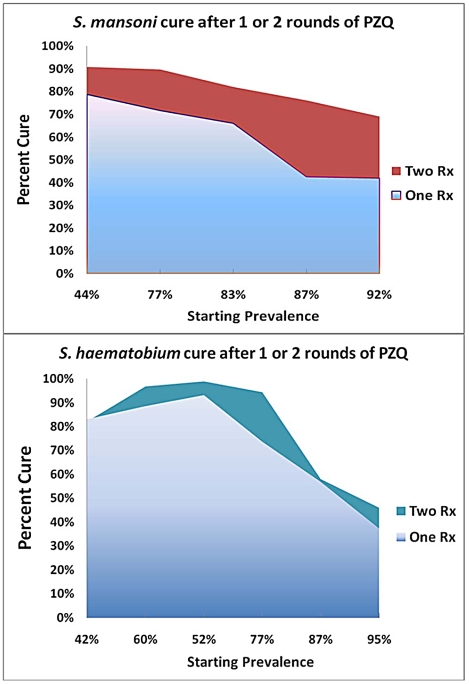
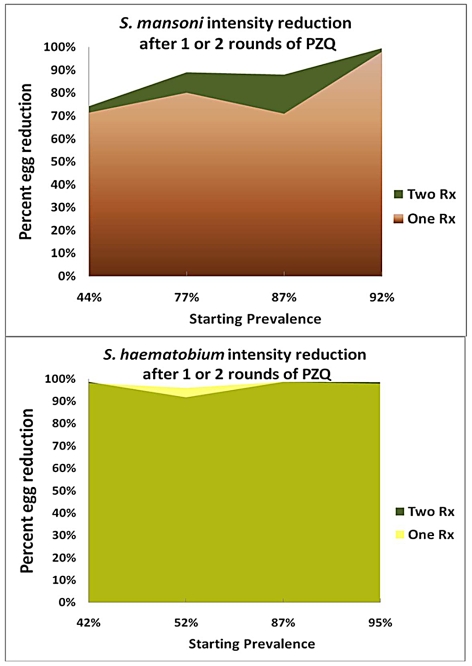
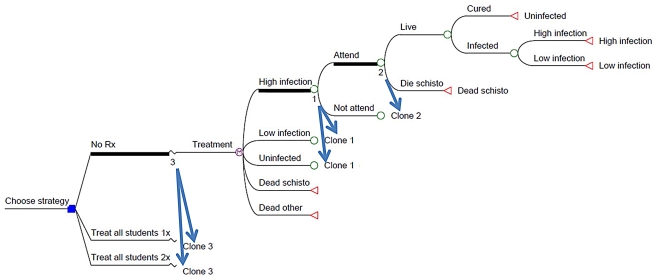
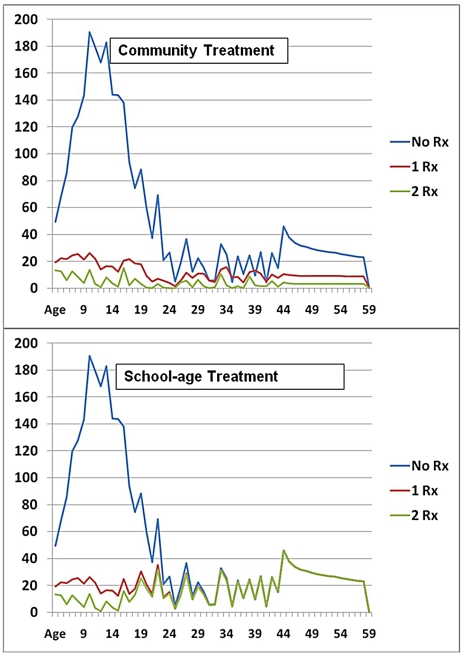
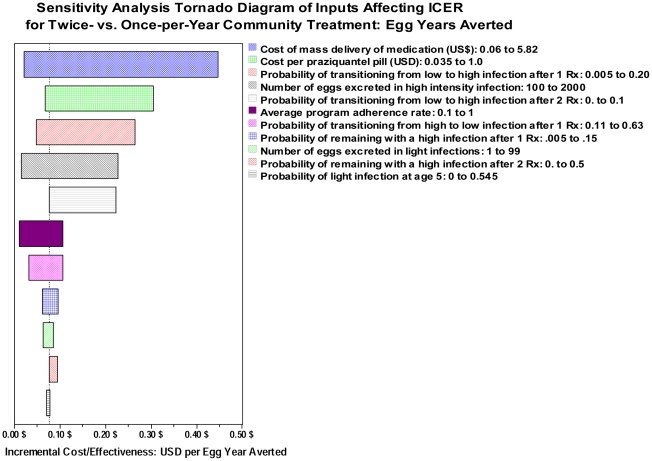
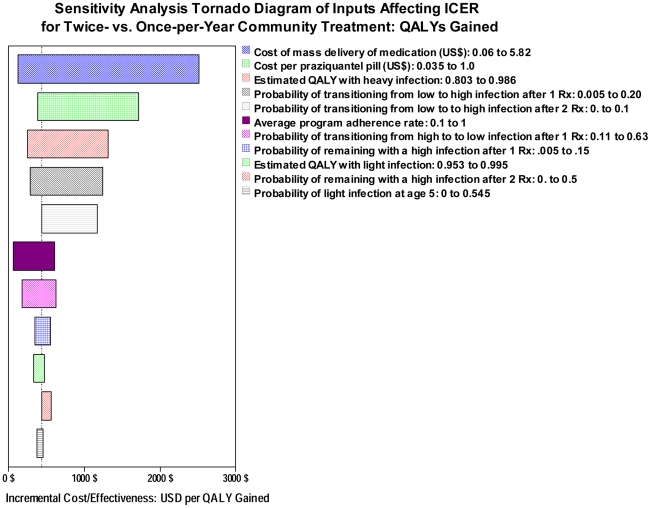
Methodology/principal findings: We performed systematic searches of electronic databases PubMed and EMBASE for relevant data using search terms 'schistosomiasis', 'dosing' and 'praziquantel' and hand searches of personal collections and bibliographies of recovered articles. In 10 reports meeting study criteria, improvements in parasitological treatment outcomes after two doses of praziquantel were greater for S. mansoni infection than for S. haematobium infection. Observed cure rates (positive to negative conversion in egg detection assays) were, for S. mansoni, 69-91% cure after two doses vs. 42-79% after one dose and, for S. haematobium, 46-99% cure after two doses vs. 37-93% after a single dose. Treatment benefits in terms of reduction in intensity (mean egg count) were also different for the two species-for S. mansoni, the 2-dose regimen yielded an weighted average 89% reduction in standardized egg counts compared to a 83% reduction after one dose; for S. haematobium, two doses gave a 93% reduction compared to a 94% reduction with a single dose. Cost-effectiveness analysis was performed based on Markov life path modeling.
Conclusions/significance: Although schedules for repeated treatment with praziquantel require greater inputs in terms of direct costs and community participation, there are incremental benefits to this approach at an estimated cost of $153 (S. mansoni)-$211 (S. haematobium) per additional lifetime QALY gained by double treatment in school-based programs. More rapid reduction of infection-related disease may improve program adherence, and if, as an externality of the program, transmission can be reduced through more effective coverage, significant additional benefits are expected to accrue in the targeted communities.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. Preventive Chemotherapy Databank [online]. 2009. Available from URL: http://www.who.int/neglected_diseases/preventive_chemotherapy/databank/e... [Accessed 2011 Aug 3]
-
- van der Werf MJ, de Vlas SJ. Morbidity and infection with schistosomes or soil-transmitted helminths. Report for WHO Parasitic Diseases and Vector Contol. Rotterdam: Erasmus University; 2001. pp. 1–103.
-
- King CH, Mahmoud AA. Drugs five years later: praziquantel. Ann Intern Med. 1989;110:290–296. - PubMed
-
- Fenwick A, Webster JP, Bosque-Oliva E, Blair L, Fleming FM, et al. The Schistosomiasis Control Initiative (SCI): rationale, development and implementation from 2002–2008. Parasitology. 2009;136:1719–1730. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
