

Outcome effectiveness of the severe sepsis resuscitation bundle with addition of lactate clearance as a bundle item: a multi-national evaluation
- PMID: 21951322
- PMCID: PMC3334775
- DOI: 10.1186/cc10469
Outcome effectiveness of the severe sepsis resuscitation bundle with addition of lactate clearance as a bundle item: a multi-national evaluation
Abstract
Introduction: Implementation of the Surviving Sepsis Campaign (SSC) guidelines has been associated with improved outcome in patients with severe sepsis. Resolution of lactate elevations or lactate clearance has also been shown to be associated with outcome. The purpose of the present study was to examine the compliance and effectiveness of the SSC resuscitation bundle with the addition of lactate clearance.
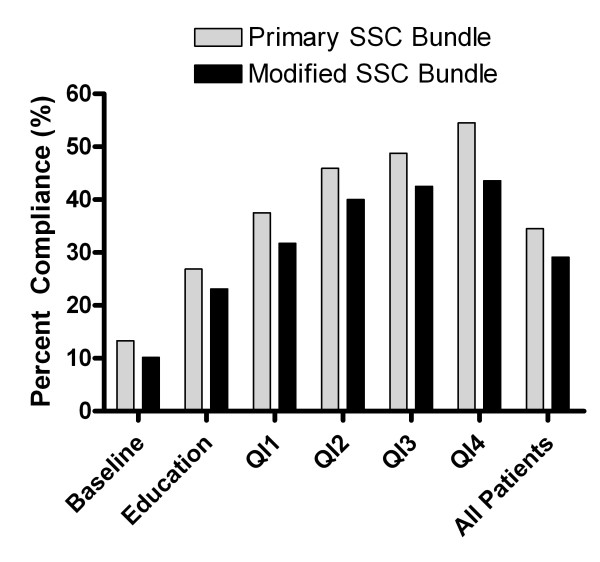
Methods: This was a prospective cohort study over 18 months in eight tertiary-care medical centers in Asia, enrolling adult patients meeting criteria for the SSC resuscitation bundle in the emergency department. Compliance and outcome results of a multi-disciplinary program to implement the Primary SSC Bundle with the addition of lactate clearance (Modified SSC Bundle) were examined. The implementation period was divided into quartiles, including baseline, education and four quality improvement phases.
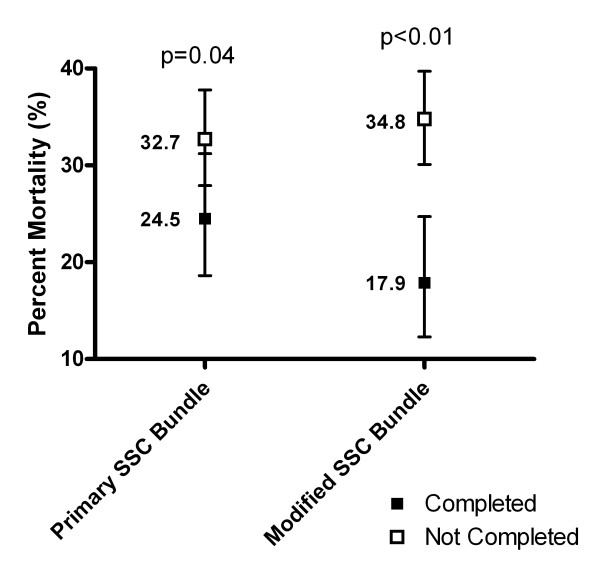
Results: A total of 556 patients were enrolled, with median (25th to 75th percentile) age 63 (50 to 74) years, lactate 4.1 (2.2 to 6.3) mmol/l, central venous pressure 10 (7 to 13) mmHg, mean arterial pressure (MAP) 70 (56 to 86) mmHg, and central venous oxygen saturation 77 (69 to 82)%. Completion of the Primary SSC Bundle over the six quartiles was 13.3, 26.9, 37.5, 45.9, 48.8, and 54.5%, respectively (P <0.01). The Modified SSC Bundle was completed in 10.2, 23.1, 31.7, 40.0, 42.5, and 43.6% patients, respectively (P <0.01). The ratio of the relative risk of death reduction for the Modified SSC Bundle compared with the Primary SSC Bundle was 1.94 (95% confidence interval = 1.45 to 39.1). Logistic regression modeling showed that the bundle items of fluid bolus given, achieve MAP >65 mmHg by 6 hours, and lactate clearance were independently associated with decreased mortality - having odds ratios (95% confidence intervals) 0.47 (0.23 to 0.96), 0.20 (0.07 to 0.55), and 0.32 (0.19 to 0.55), respectively.
Conclusions: The addition of lactate clearance to the SSC resuscitation bundle is associated with improved mortality. In our study patient population with optimized baseline central venous pressure and central venous oxygen saturation, the bundle items of fluid bolus administration, achieving MAP >65 mmHg, and lactate clearance were independent predictors of outcome.
Figures
Comment in
-
The role of lactate clearance in the resuscitation bundle.Crit Care. 2011;15(5):199. doi: 10.1186/cc10478. Epub 2011 Oct 24. Crit Care. 2011. PMID: 22078132 Free PMC article.
References
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296–327. doi: 10.1097/01.CCM.0000298158.12101.41. - DOI - PubMed
-
- Ferrer R, Artigas A, Levy MM, Blanco J, Gonzalez-Diaz G, Garnacho-Montero J, Ibanez J, Palencia E, Quintana M, de la Torre-Prados MV. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA. 2008;299:2294–2303. doi: 10.1001/jama.299.19.2294. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
