

A maternal erythrocyte DHA content of approximately 6 g% is the DHA status at which intrauterine DHA biomagnifications turns into bioattenuation and postnatal infant DHA equilibrium is reached
- PMID: 21952690
- PMCID: PMC3419349
- DOI: 10.1007/s00394-011-0245-9
A maternal erythrocyte DHA content of approximately 6 g% is the DHA status at which intrauterine DHA biomagnifications turns into bioattenuation and postnatal infant DHA equilibrium is reached
Abstract
Purpose: Higher long-chain polyunsaturated fatty acids (LCP) in infant compared with maternal lipids at delivery is named biomagnification. The decline of infant and maternal docosahexaenoic acid (DHA) status during lactation in Western countries suggests maternal depletion. We investigated whether biomagnification persists at lifelong high fish intakes and whether the latter prevents a postpartum decline of infant and/or maternal DHA status.
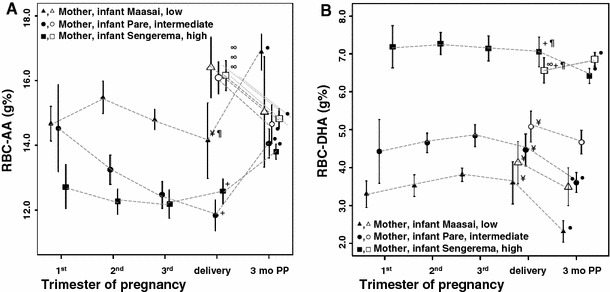
Methods: We studied 3 Tanzanian tribes with low (Maasai: 0/week), intermediate (Pare: 2-3/week), and high (Sengerema: 4-5/week) fish intakes. DHA and arachidonic acid (AA) were determined in maternal (m) and infant (i) erythrocytes (RBC) during pregnancy (1st trimester n = 14, 2nd = 103, 3rd = 88), and in mother-infant pairs at delivery (n = 63) and at 3 months postpartum (n = 104).
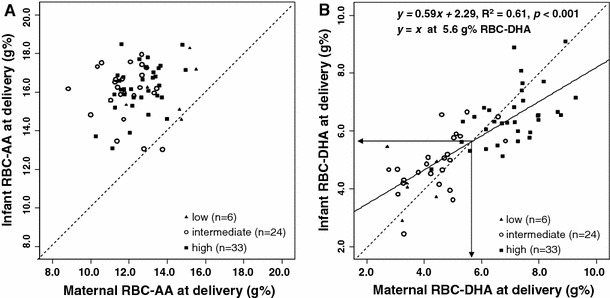
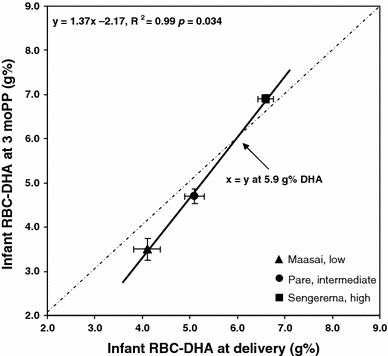
Results: At delivery, infants of all tribes had similar iRBC-AA which was higher than, and unrelated to, mRBC-AA. Transplacental DHA biomagnification occurred up to 5.6 g% mRBC-DHA; higher mRBC-DHA was associated with "bioattenuation" (i.e., iRBC-DHA < mRBC-DHA). Compared to delivery, mRBC-AA after 3 months was higher, while iRBC-AA was lower. mRBC-DHA after 3 months was lower, while iRBC-DHA was lower (low fish intake), equal (intermediate fish intake), and higher (high fish intake) compared to delivery. We estimated that postpartum iRBC-DHA equilibrium is reached at 5.9 g%, which corresponds to a mRBC-DHA of 6.1 g% throughout pregnancy.
Conclusion: Uniform high iRBC-AA at delivery might indicate the importance of intrauterine infant AA status. Biomagnification reflects low maternal DHA status, and bioattenuation may prevent intrauterine competition of DHA with AA. A mRBC-DHA of about 6 g% during pregnancy predicts maternal-fetal equilibrium at delivery, postnatal iRBC-DHA equilibrium, but is unable to prevent a postnatal mRBC-DHA decline.
Figures
References
-
- Kuipers RS, Fokkema MR, Smit EN, van der Meulen J, Boersma ER, Muskiet FA. High contents of both docosahexaenoic and arachidonic acids in milk of women consuming fish from lake Kitangiri (Tanzania): targets for infant formulae close to our ancient diet? Prostaglandins Leukot Essent Fatty Acids. 2005;72:279–288. doi: 10.1016/j.plefa.2004.12.001. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
