

Hepatocellular carcinoma confirmation, treatment, and survival in surveillance, epidemiology, and end results registries, 1992-2008
- PMID: 21953588
- PMCID: PMC3868012
- DOI: 10.1002/hep.24710
Hepatocellular carcinoma confirmation, treatment, and survival in surveillance, epidemiology, and end results registries, 1992-2008
Abstract
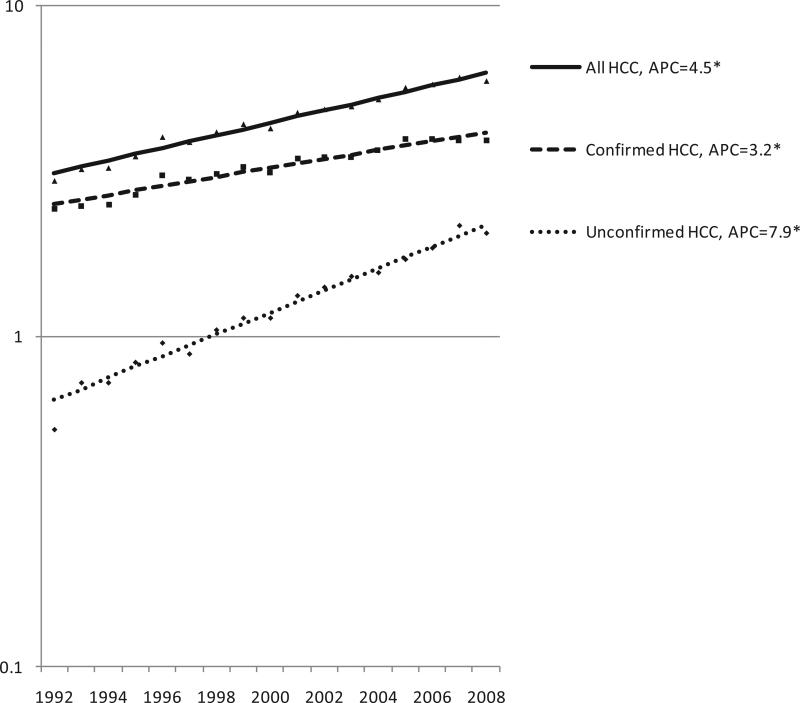
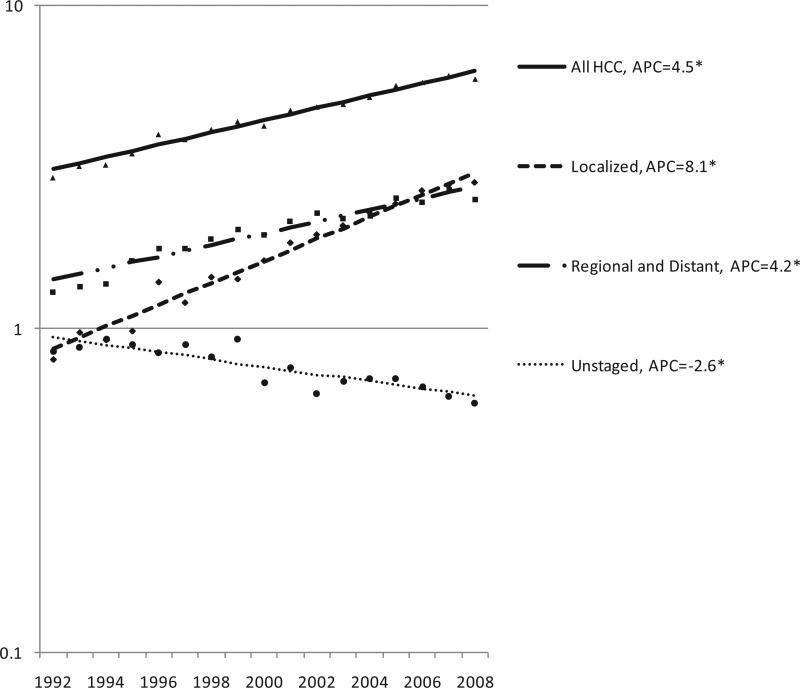
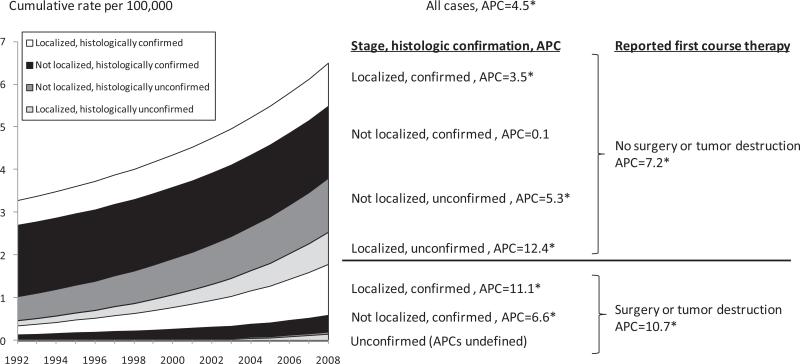
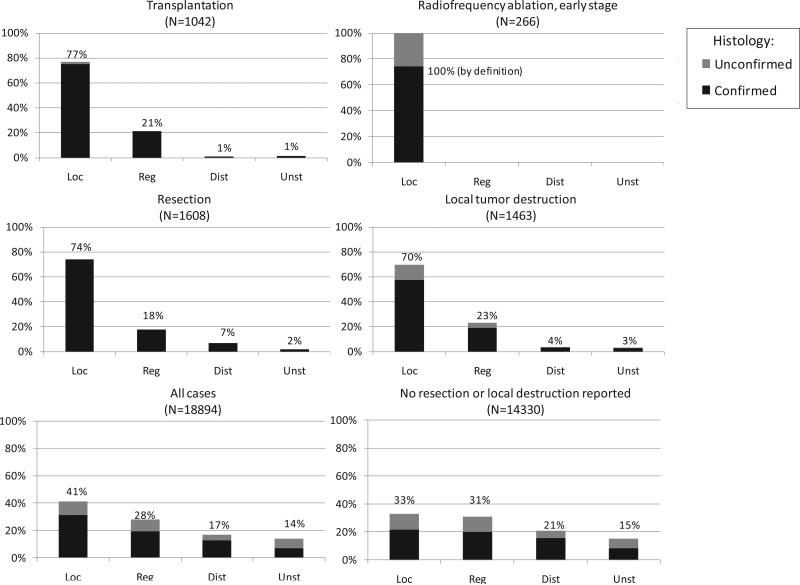
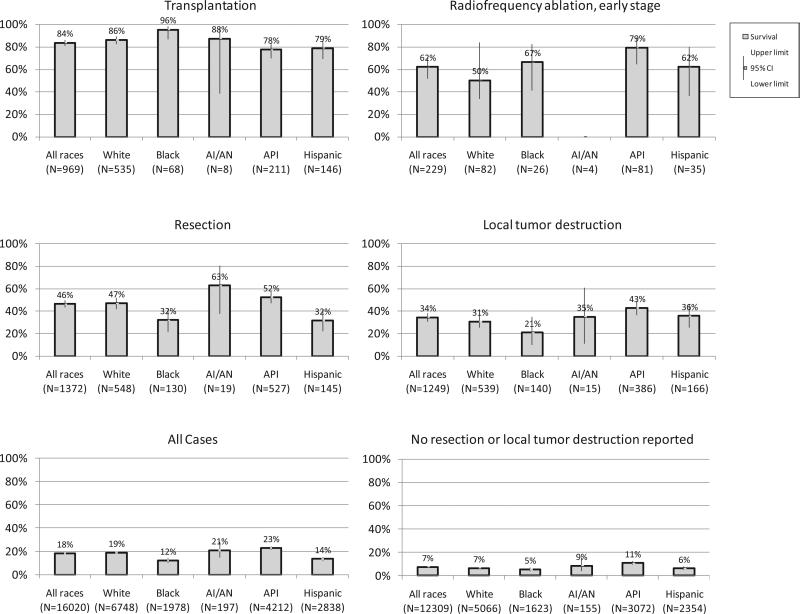
Approaches to the diagnosis and management of hepatocellular carcinoma (HCC) are improving survival. In the Surveillance, Epidemiology, and End Results-13 registries, HCC stage, histological confirmation, and first-course surgery were examined. Among 21,390 HCC cases diagnosed with follow-up of vital status during 1998-2008, there were 4,727 (22%) with reported first-course invasive liver surgery, local tumor destruction, or both. The proportion with reported liver surgery or ablation was 39% among localized stage cases and only 4% among distant/unstaged cases. Though 70% of cases had histologically confirmed diagnoses, the proportion with confirmed diagnoses was higher among cases with reported invasive surgery (99%), compared to cases receiving ablation (81%) or no reported therapy (65%). Incidence rates of histologically unconfirmed HCC increased faster than those of confirmed HCC from 1992 to 2008 (8% versus 3% per year). Two encouraging findings were that incidence rates of localized-stage HCC increased faster than rates of regional- and distant-stage HCC combined (8% versus 4% per year), and that incidence rates of reported first-course surgery or tumor destruction increased faster than incidence rates of HCC without such therapy (11% versus 7%). Between 1975-1977 and 1998-2007, 5-year cause-specific HCC survival increased from just 3% to 18%. Survival was 84% among transplant recipients, 53% among cases receiving radiofrequency ablation at early stage, 47% among cases undergoing resection, and 35% among cases receiving local tumor destruction. Asian or Pacific Islander cases had significantly better 5-year survival (23%) than white (18%), Hispanic (15%), or black cases (12%).
Conclusion: HCC survival is improving, because more cases are diagnosed and treated at early stages. Additional progress may be possible with continued use of clinical surveillance to follow individuals at risk for HCC, enabling early intervention.
Copyright © 2011 American Association for the Study of Liver Diseases.
Figures
References
-
- Ahmed F, Perz JF, Kwong S, Jamison PM, Friedman C, Bell BP. National trends and disparities in the incidence of hepatocellular carcinoma, 1998-2003. [May 17, 2011];Prev Chronic Dis. 2008 :5. http://www.cdc.gov/pcd/issues/2008/jul/07_0155.htm. - PMC - PubMed
-
- El-Serag HB, Marrero JA, Rudolph L, et al. Diagnosis and treatment of hepatocellular carcinoma. Gastroenterology. 2008;134:1752–1763. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical