

Prescribing practices in a US cohort of rheumatoid arthritis patients before and after publication of the American College of Rheumatology treatment recommendations
- PMID: 21953645
- PMCID: PMC3253907
- DOI: 10.1002/art.33380
Prescribing practices in a US cohort of rheumatoid arthritis patients before and after publication of the American College of Rheumatology treatment recommendations
Abstract
Objective: To examine prescribing practices in the use of biologic and nonbiologic disease-modifying antirheumatic drugs (DMARDs) to treat patients with rheumatoid arthritis (RA), before and after publication of the American College of Rheumatology (ACR) treatment recommendations.
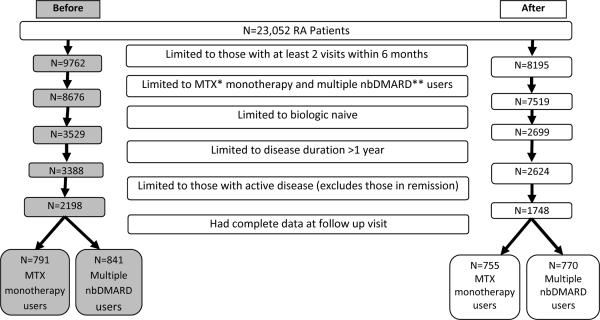
Methods: Biologics-naive RA patients under the care of a rheumatologist in the US were identified from the Consortium of Rheumatology Researchers of North America registry. Patients were included if their visits occurred prior to and/or at least 6 months after publication of the ACR treatment recommendations (time periods of February 2002-June 2008 versus December 2008-December 2009). The population was divided into 2 mutually exclusive cohorts: 1) methotrexate (MTX) monotherapy users, and 2) multiple nonbiologic DMARD users. Initiation or dose escalation of biologic and nonbiologic DMARDs in response to active disease was assessed cross-sectionally and longitudinally in comparison to the ACR recommendations. The impact of the publication of the ACR recommendations on treatment practices was assessed using logistic regression, stratified by disease activity and adjusted for clustering of physicians and geographic region.
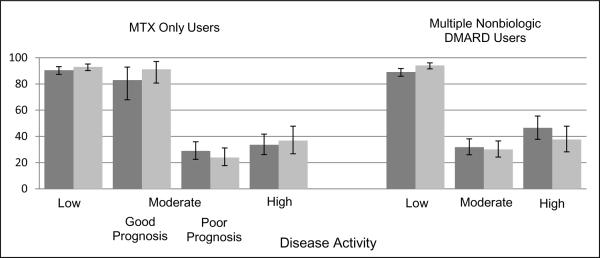
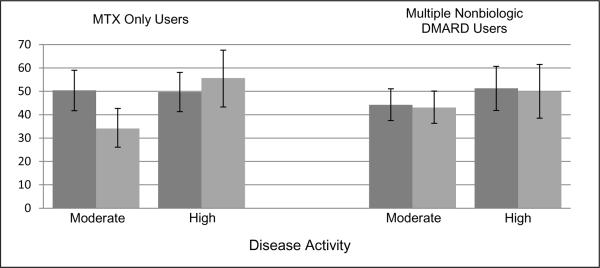
Results: After 1 visit, 24-37% of patients receiving MTX monotherapy who had moderate disease activity and a poor prognosis or high disease activity received care consistent with the ACR recommendations; after 2 visits, 34-56% of the MTX monotherapy group received care consistent with the recommendations. In the patients receiving multiple nonbiologic DMARDs, 31-47% of those with moderate or high disease activity received care consistent with the recommendations after 1 visit, and 43-51% received such care after 2 visits. Publication of the recommendations did not significantly change treatment patterns for those with active disease.
Conclusion: Substantial numbers of RA patients with active disease did not receive care consistent with the current ACR treatment recommendations. Innovative approaches to improve care are necessary.
Copyright © 2012 by the American College of Rheumatology.
Figures
References
-
- Helmick CG, Felson DT, Lawrence RC, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis & Rheumatism. 2008;58(1):15–25. - PubMed
-
- Smolen JS, Aletaha D, Machold KP. Therapeutic strategies in early rheumatoid arthritis. Best Practice & Research Clinical Rheumatology. 2005;19(1):163–77. - PubMed
-
- van Vollenhoven RF, Ernestam S, Geborek P, et al. Addition of infliximab compared with addition of sulfasalazine and hydroxychloroquine to methotrexate in patients with early rheumatoid arthritis (Swefot trial): 1-year results of a randomised trial. Lancet. 2009;374(9688):459–66. - PubMed
-
- Saag KG, Teng GG, Patkar NM, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59(6):762–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
