

Evaluation of nonfasting tests to screen for childhood and adolescent dysglycemia
- PMID: 21953800
- PMCID: PMC3220868
- DOI: 10.2337/dc11-0827
Evaluation of nonfasting tests to screen for childhood and adolescent dysglycemia
Abstract
Objective: To assess performance of nonfasting tests to screen children for dysglycemia (prediabetes or diabetes).
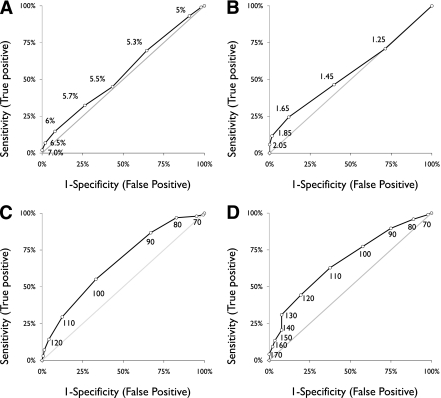
Research design and methods: This was a cross-sectional study of 254 overweight or obese (BMI ≥85th percentile) children aged 10-17 years. Subjects came for two visits to a clinical research unit. For visit one, they arrived fasting and a 2-h glucose tolerance test and HbA(1c) and fructosamine testing were performed. For visit two, they arrived nonfasting and had a random plasma glucose, a 1-h 50-g nonfasting glucose challenge test (1-h GCT), and urine dipstick performed. The primary end point was dysglycemia (fasting plasma glucose ≥100 mg/dL or a 2-h postglucose ≥140 mg/dL). Test performance was assessed using receiver operating characteristic (ROC) curves and calculations of area under the ROC curve.
Results: Approximately one-half of children were female, 59% were white, and 30% were black. There were 99 (39%) cases of prediabetes and 3 (1.2%) cases of diabetes. Urine dipstick, HbA(1c) (area under the curve [AUC] 0.54 [95% CI 0.47-0.61]), and fructosamine (AUC 0.55 [0.47-0.63]) displayed poor discrimination for identifying children with dysglycemia. Both random glucose (AUC 0.66 [0.60-0.73]) and 1-h GCT (AUC 0.68 [0.61-0.74]) had better levels of test discrimination than HbA(1c) or fructosamine.
Conclusions: HbA(1c) had poor discrimination, which could lead to missed cases of dysglycemia in children. Random glucose or 1-h GCT may potentially be incorporated into clinical practice as initial screening tests for prediabetes or diabetes and for determining which children should undergo further definitive testing.
Figures
References
-
- Pinhas-Hamiel O, Dolan LM, Daniels SR, Standiford D, Khoury PR, Zeitler P. Increased incidence of non-insulin-dependent diabetes mellitus among adolescents. J Pediatr 1996;128:608–615 - PubMed
-
- Lipton RB, Drum M, Burnet D, et al. Obesity at the onset of diabetes in an ethnically diverse population of children: what does it mean for epidemiologists and clinicians? Pediatrics 2005;115:e553–e560 - PubMed
-
- American Diabetes Association Type 2 diabetes in children and adolescents. Pediatrics 2000;105:671–680 - PubMed
-
- Krebs NF, Himes JH, Jacobson D, Nicklas TA, Guilday P, Styne D. Assessment of child and adolescent overweight and obesity. Pediatrics 2007;120(Suppl. 4):S193–S228 - PubMed
-
- Kaufman FR. Type 2 diabetes in children and youth. Rev Endocr Metab Disord 2003;4:33–42 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
