

LDL-apheresis depletes apoE-HDL and pre-β1-HDL in familial hypercholesterolemia: relevance to atheroprotection
- PMID: 21957200
- PMCID: PMC3283261
- DOI: 10.1194/jlr.P016816
LDL-apheresis depletes apoE-HDL and pre-β1-HDL in familial hypercholesterolemia: relevance to atheroprotection
Abstract
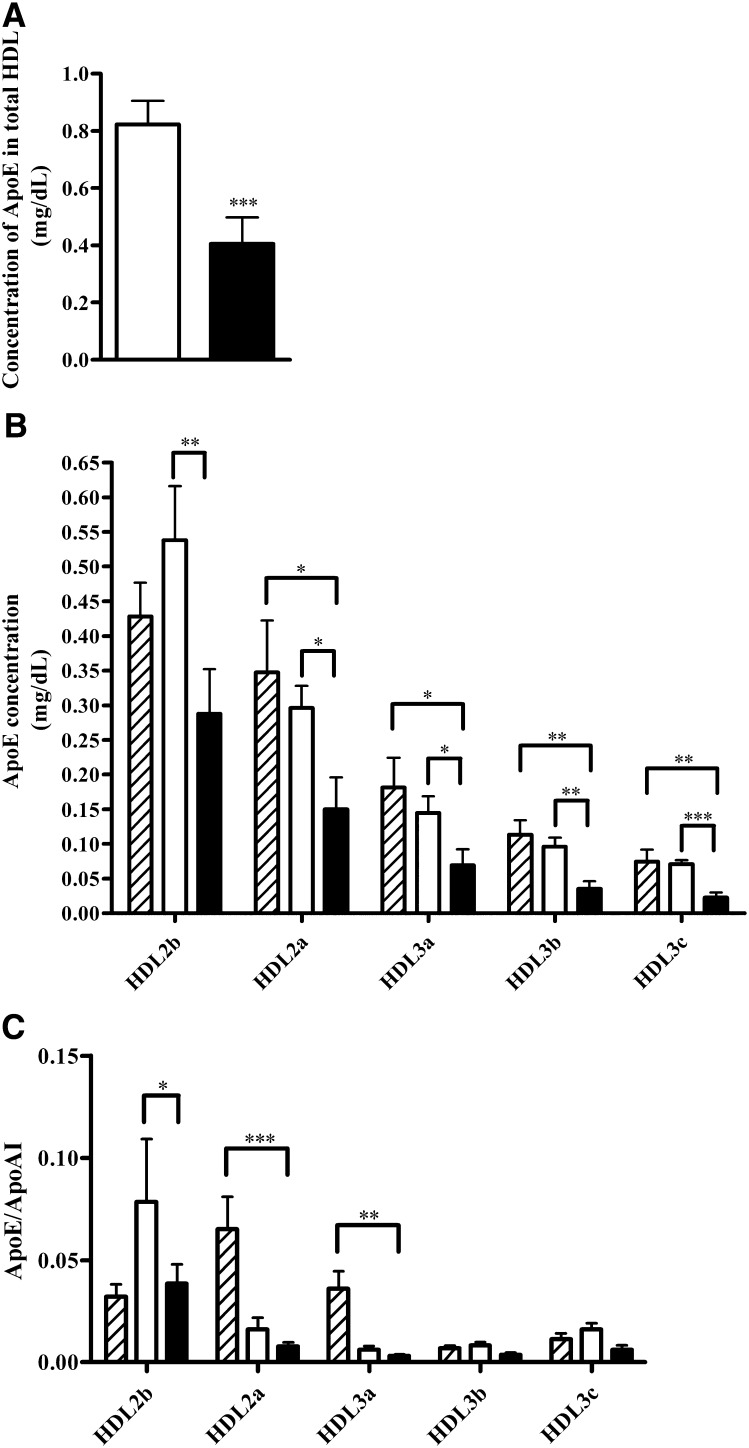
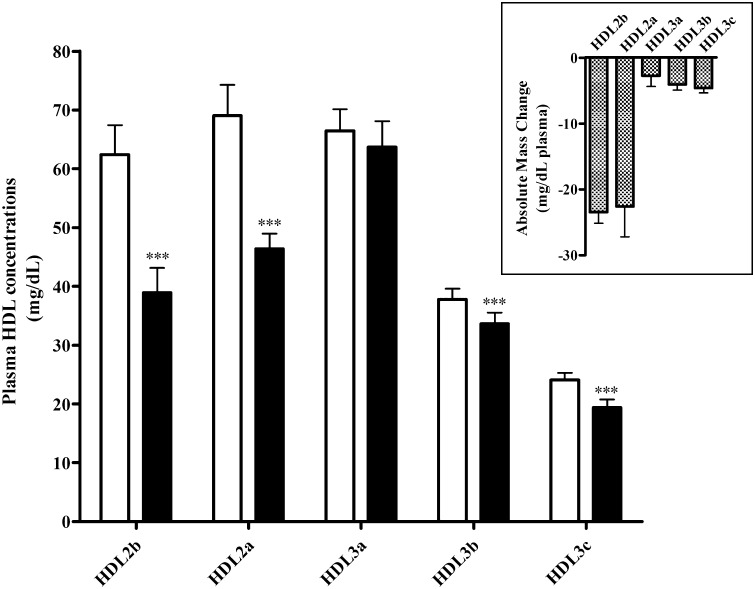
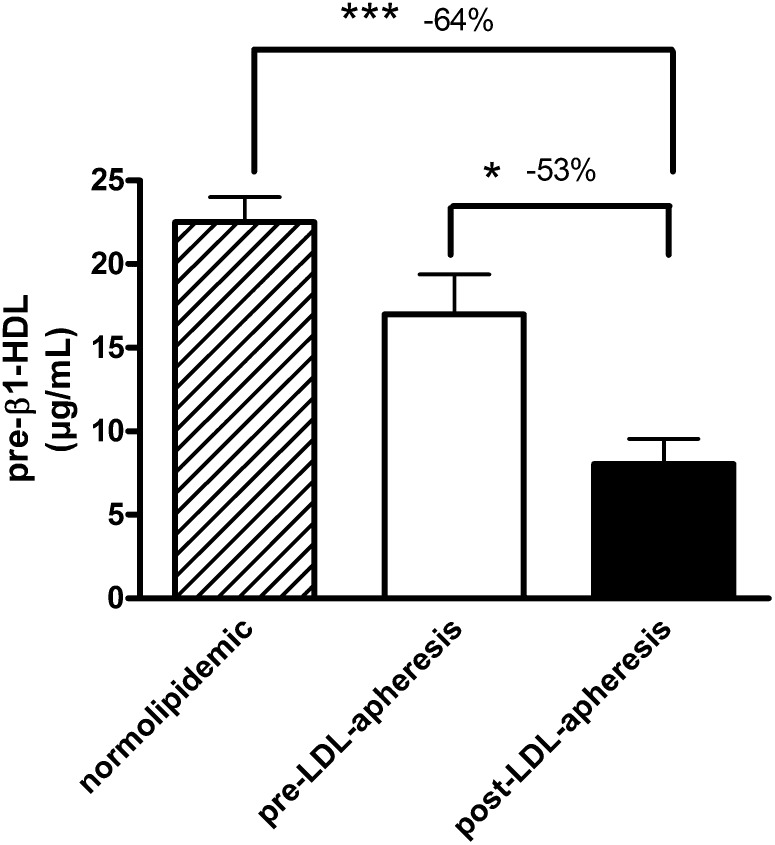
Subnormal HDL-cholesterol (HDL-C) and apolipoprotein (apo)AI levels are characteristic of familial hypercholesterolemia (FH), reflecting perturbed intravascular metabolism with compositional anomalies in HDL particles, including apoE enrichment. Does LDL-apheresis, which reduces HDL-cholesterol, apoAI, and apoE by adsorption, induce selective changes in HDL subpopulations, with relevance to atheroprotection? Five HDL subpopulations were fractionated from pre- and post-LDL-apheresis plasmas of normotriglyceridemic FH subjects (n = 11) on regular LDL-apheresis (>2 years). Apheresis lowered both plasma apoE (-62%) and apoAI (-16%) levels, with preferential, genotype-independent reduction in apoE. The mass ratio of HDL2:HDL3 was lowered from ~1:1 to 0.72:1 by apheresis, reflecting selective removal of HDL2 mass (80% of total HDL adsorbed). Pre-LDL-apheresis, HDL2 subpopulations were markedly enriched in apoE, consistent with ~1 copy of apoE per 4 HDL particles. Large amounts (50-66%) of apoE-HDL were removed by apheresis, preferentially in the HDL2b subfraction (-50%); minor absolute amounts of apoE-HDL were removed from HDL3 subfractions. Furthermore, pre-β1-HDL particle levels were subnormal following removal (-53%) upon apheresis, suggesting that cellular cholesterol efflux may be defective in the immediate postapheresis period. In LDL-receptor (LDL-R) deficiency, LDL-apheresis may enhance flux through the reverse cholesterol transport pathway and equally attenuate potential biglycan-mediated deposition of apoE-HDL in the arterial matrix.
Figures
References
-
- Goldstein J. L., Hobbs H. H., Brown M. S. 2001. Familial hypercholesterolemia. The Metabolic Basis of Inherited Disease. Scriver C. R., Beaudet A. L., Sly W. S., Valle D., McGraw-Hill, New York: 2863–2913.
-
- Gordon D. J., Probstfield J. L., Garrison R. J., Neaton J. D., Castelli W. P., Knoke J. D., Jacobs D. R., Bangdiwala S., Tyroler H. A. 1989. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation. 79: 8–15. - PubMed
-
- Chapman M. J., Ginsberg H. N., Amarenco P., Andreotti F., Borén J., Catapano A. L., Descamps O. S., Fisher E., Kovanen P. T., Kuivenhoven J. A., et al. 2011. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management. Eur. Heart J. 32: 1345–1361. - PMC - PubMed
-
- Bellanger N., Orsoni A., Julia Z., Fournier N., Frisdal E., Duchene E., Bruckert E., Carrie A., Bonnefont-Rousselot D., Pirault J., et al. 2011. Atheroprotective reverse cholesterol transport pathway is defective in familial hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 31: 1675–1681. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
