

Postoperative chemoradiation for resected gastric cancer--is the Macdonald Regimen Tolerable? a retrospective multi-institutional study
- PMID: 21958692
- PMCID: PMC3219562
- DOI: 10.1186/1748-717X-6-127
Postoperative chemoradiation for resected gastric cancer--is the Macdonald Regimen Tolerable? a retrospective multi-institutional study
Abstract
Background: Postoperative chemoradiation as per Intergroup-0116 trial ("Macdonald regimen") is considered standard for completely resected high risk gastric cancer. However, many concerns remain with regards to the toxicity of this regimen. To evaluate the safety and tolerability of this regimen in a routine clinical practice setting, we analyzed our experience with its use. As we did not expect a different toxic profile in patients (pts) with positive margins (R1 resection), these were studied together with pts after complete resection (R0).
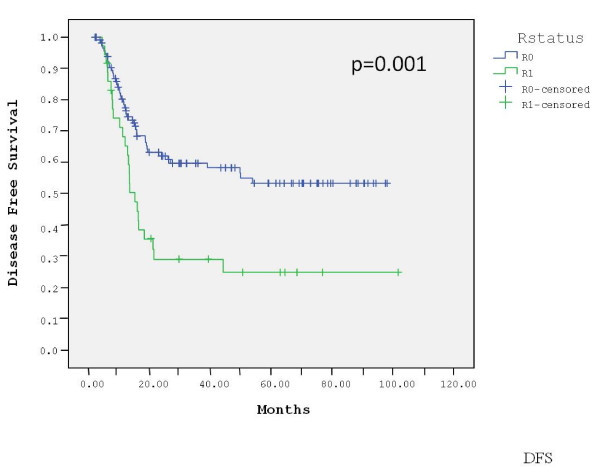
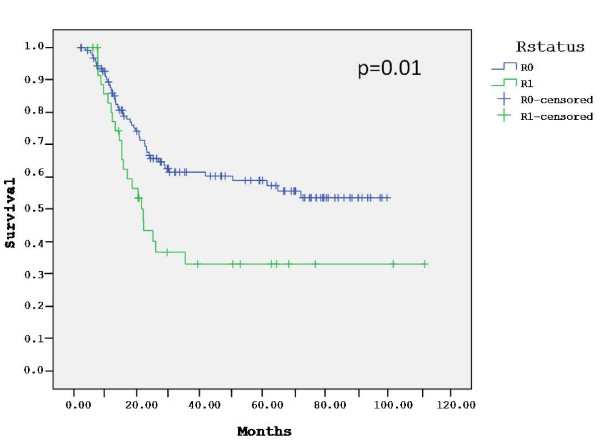
Patients and methods: Postoperative chemoradiation therapy was given according to the original Intergroup-0116 regimen. Overall survival (OS) and disease free survival (DFS) rates were calculated using the Kaplan-Meier method. Comparison of OS and DFS between R0 and R1 pts was done using the log-rank test.
Results: Between 6/2000 and 12/2007, 166 pts after R0 (129 pts) or R1 (37 pts) resection of locally advanced gastric adenocarcinoma received postoperative chemoradiation; 61% were male and the median age was 63 years (range, 23-86); 78% had T ≥ 3 tumors and 81% had N+ disease; 87% of the pts completed radiotherapy and 54% completed the entire chemoradiation plan; 46.4% had grade ≥ 3 toxicity and 32% were hospitalized at least once for toxicity. Three pts (1.8%) died of toxicity: diarrhea (1), neutropenic sepsis (1) and neutropenic sepsis complicated by small bowel gangrene (1). The most common hematological toxicity was neutropenia, grade ≥ 3 in 30% of pts and complicated by fever in 15%. The most common non-hematological toxicities were nausea, vomiting and diarrhea. With a median follow-up of 51 months (range, 2-100), 62% of the R0 patients remain alive and 61% are free of disease. Median DFS and OS for R0 were not reached. R0 pts had a significantly higher 3-year DFS (60% vs. 29%, p = 0.001) and OS (61% vs. 33%, p = 0.01) compared with R1 pts.
Conclusions: In our experience, postoperative chemoradiation as per Intergroup-0116 seems to be substantially toxic, with a mortality rate which seems higher than reported in that trial. Efficacy data appears comparable to the original report. Following postoperative chemoradiation, involvement of surgical margins still has a detrimental impact on patient outcome.
Figures
References
-
- Garcia M, Ward EM, Center MM, Hao Y, Siegel RL, Thun MJ. Global Cancer Facts & Figures. 2007. http://www.cancer.gov [online]. Accessed Aug 20, 2008.
-
- Landry J, Tepper JE, Wood WC, Moulton EO, Koerner F, Sullinger J. Patterns of failure following curative resection of gastric cancer. Int J Radiat Oncol Biol Phys. 1990;191:1357–1362. - PubMed
-
- Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or Gastroesophageal junction. N Engl J Med. 2001;345:725–730. doi: 10.1056/NEJMoa010187. - DOI - PubMed
-
- Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual. 7. New York: Springer-Verlag; 2010. pp. 145–147.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
