

Mechanical property and tissue mineral density differences among severely suppressed bone turnover (SSBT) patients, osteoporotic patients, and normal subjects
- PMID: 21958843
- PMCID: PMC3221814
- DOI: 10.1016/j.bone.2011.09.042
Mechanical property and tissue mineral density differences among severely suppressed bone turnover (SSBT) patients, osteoporotic patients, and normal subjects
Abstract
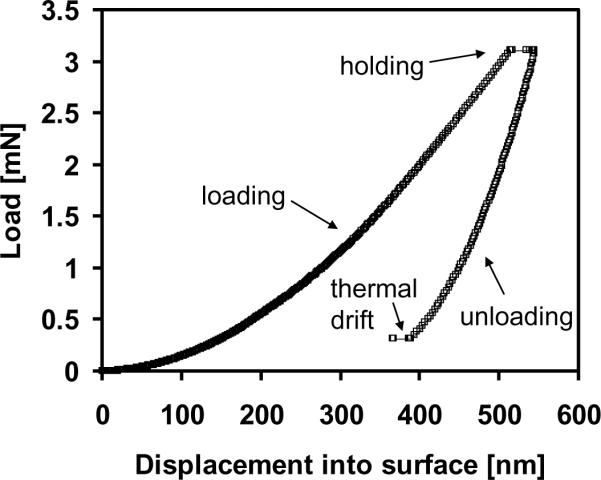
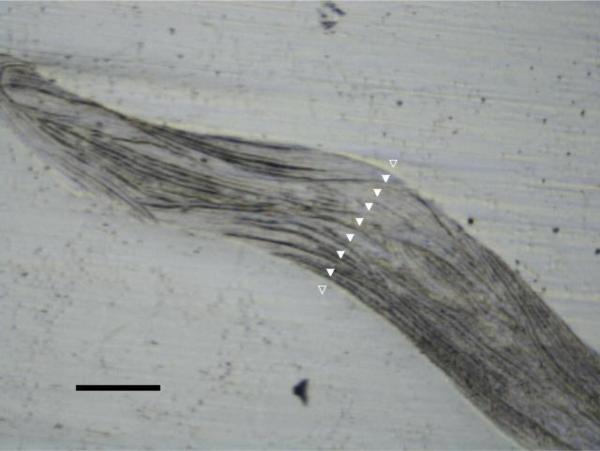
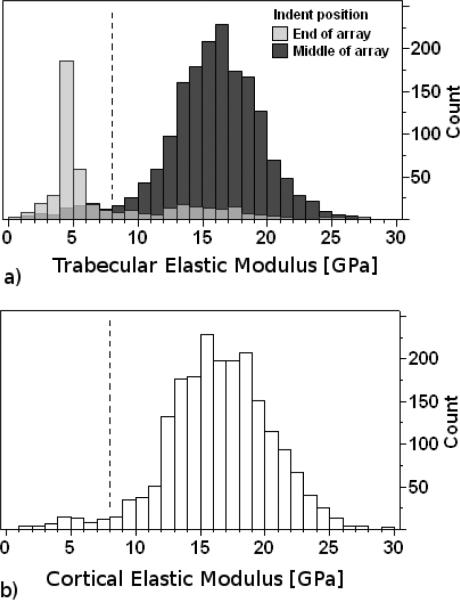
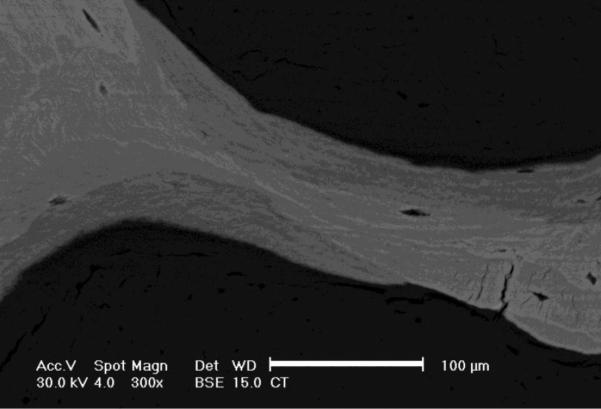
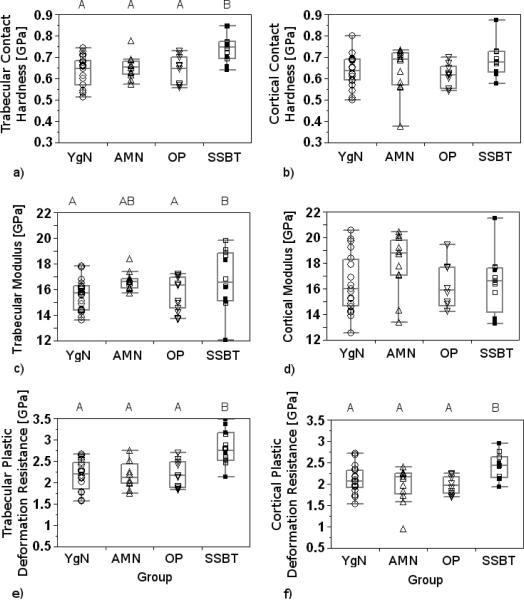
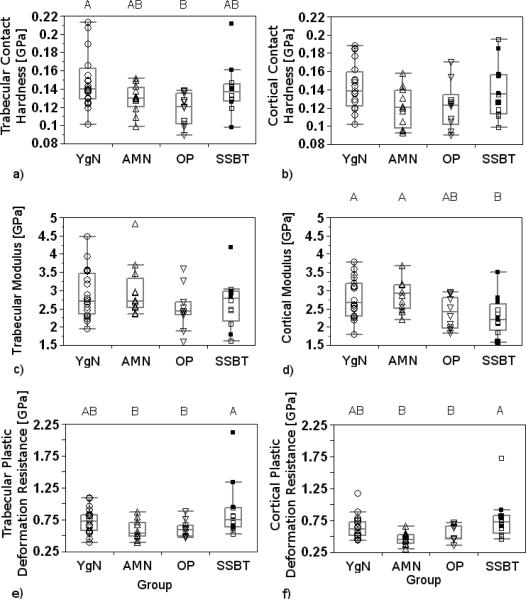
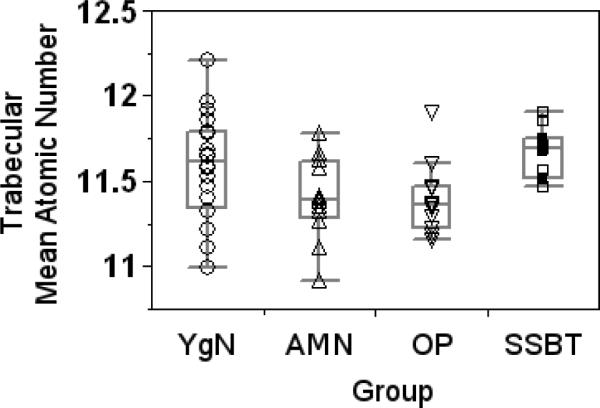
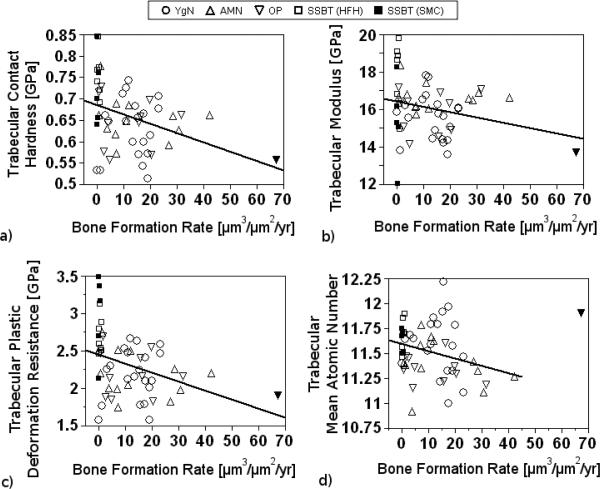
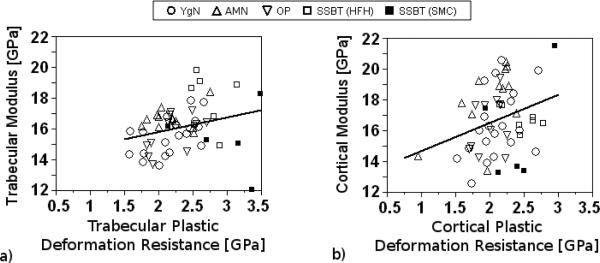
Pathogenesis of atypical fractures in patients on long term bisphosphonate therapy is poorly understood, and the type, the manner in which they occur and the fracture sites are quite different from the usual osteoporotic fractures. We hypothesized that the tissue-level mechanical properties and mean degree of mineralization of the iliac bone would differ among 1) patients with atypical fractures and severely suppressed bone turnover (SSBT) associated with long-term bisphosphonate therapy, 2) age-matched, treatment-naïve osteoporotic patients with vertebral fracture, 3) age-matched normals and 4) young normals. Large differences in tissue-level mechanical properties and/or mineralization among these groups could help explain the underlying mechanism(s) for the occurrence of typical osteoporotic and the atypical femoral shaft fractures. Elastic modulus, contact hardness, plastic deformation resistance, and tissue mineral densities of cortical and trabecular bone regions of 55 iliac bone biopsies--12 SSBT patients (SSBT; aged 49-77), 11 age-matched untreated osteoporotic patients with vertebral fracture (Osteoporotic), 12 age-matched subjects without bone fracture (Age-Matched Normal), and 20 younger subjects without bone fracture (Young Normal)--were measured using nanoindentation and quantitative backscattered electron microscopy. For cortical bone nanoindentation properties, only plastic deformation resistance was different among the groups (p<0.05), with greater resistance to plastic deformation in the SSBT group compared to all other groups. For trabecular bone, all nanoindentation properties and mineral density of the trabecular bone were different among the groups (p<0.05). The SSBT group had greater plastic deformation resistance and harder trabecular bone compared to the other three groups, stiffer bone compared to the Osteoporotic and Young Normal groups, and a trend of higher mineral density compared to the Age-Matched Normal and Osteoporotic groups. Lower heterogeneity of modulus and contact hardness for cortical bone of the SSBT and trabecular bone of the Osteoporotic fracture groups, respectively, compared to the non-fractured groups, may contribute to fracture susceptibility due to lowered ability to prevent crack propagation. We tentatively conclude that, in addition to extremely low bone formation rate, atypical fractures in SSBT and/or long-term bisphosphonate treatment may be associated with greater mean plastic deformation resistance properties and less heterogeneous elastic properties of the bone.
Published by Elsevier Inc.
Figures
References
-
- Kanis JA, Melton LJ, 3rd, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994;9:1137–41. - PubMed
-
- Black DM, Kelly MP, Genant HK, Palermo L, Eastell R, Bucci-Rechtweg C, Cauley J, Leung PC, Boonen S, Santora A, de Papp A, Bauer DC. Bisphosphonates and Fractures of the Subtrochanteric or Diaphyseal Femur. N Engl J Med. 2010 - PubMed
-
- Girgis CM, Sher D, Seibel MJ. Atypical femoral fractures and bisphosphonate use. N Engl J Med. 2010;362:1848–9. - PubMed
-
- Lenart BA, Lorich DG, Lane JM. Atypical fractures of the femoral diaphysis in postmenopausal women taking alendronate. N Engl J Med. 2008;358:1304–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
