

Optical treatment of strabismic and combined strabismic-anisometropic amblyopia
- PMID: 21959371
- PMCID: PMC3250558
- DOI: 10.1016/j.ophtha.2011.06.043
Optical treatment of strabismic and combined strabismic-anisometropic amblyopia
Abstract
Objective: To determine visual acuity improvement in children with strabismic and combined strabismic-anisometropic (combined-mechanism) amblyopia treated with optical correction alone and to explore factors associated with improvement.
Design: Prospective, multicenter, cohort study.
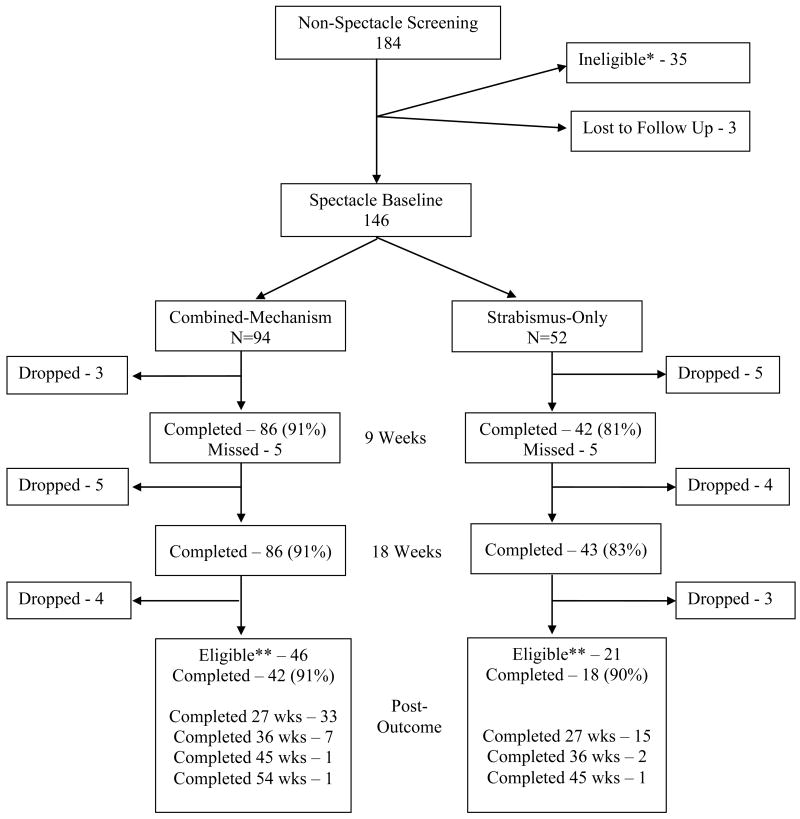
Participants: We included 146 children 3 to <7 years old with previously untreated strabismic amblyopia (n = 52) or combined-mechanism amblyopia (n = 94).
Methods: Optical treatment was provided as spectacles (prescription based on a cycloplegic refraction) that were worn for the first time at the baseline visit. Visual acuity with spectacles was measured using the Amblyopia Treatment Study HOTV visual acuity protocol at baseline and every 9 weeks thereafter until no further improvement in visual acuity. Ocular alignment was assessed at each visit.
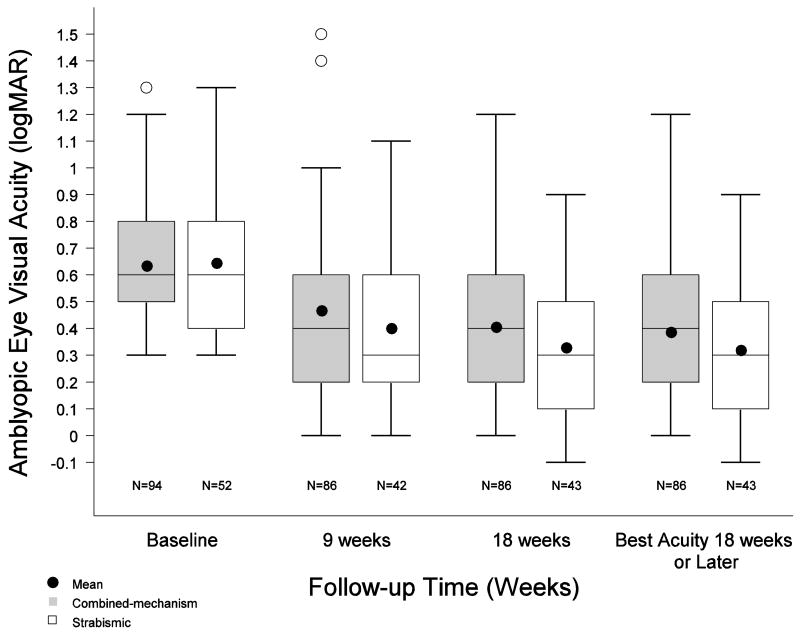
Main outcome measures: Visual acuity 18 weeks after baseline.
Results: Overall, amblyopic eye visual acuity improved a mean of 2.6 lines (95% confidence interval [CI], 2.3-3.0), with 75% of children improving ≥ 2 lines and 54% improving ≥ 3 lines. Resolution of amblyopia occurred in 32% (95% CI, 24%-41%) of the children. The treatment effect was greater for strabismic amblyopia than for combined-mechanism amblyopia (3.2 vs 2.3 lines; adjusted P = 0.003). Visual acuity improved regardless of whether eye alignment improved.
Conclusions: Optical treatment alone of strabismic and combined-mechanism amblyopia results in clinically meaningful improvement in amblyopic eye visual acuity for most 3- to <7-year-old children, resolving in at least one quarter without the need for additional treatment. Consideration should be given to prescribing refractive correction as the sole initial treatment for children with strabismic or combined-mechanism amblyopia before initiating other therapies.
Financial disclosure(s): The authors have no proprietary or commercial interest in any of the materials discussed in this article.
Copyright © 2012 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
No conflicting relationship exists for any author.
Figures
References
-
- Chen PL, Chen JT, Tai MC, et al. Anisometropic amblyopia treated with spectacle correction alone: possible factors predicting success and time to start patching. Am J Ophthalmol. 2007;143:54–60. - PubMed
-
- Agervi P, Kugelberg U, Kugelberg M, et al. Treatment of anisometropic amblyopia with spectacles or in combination with translucent Bangerter filters. Ophthalmology. 2009;116:1475–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
