

Long-term outcomes after transoral incisionless fundoplication in patients with GERD and LPR symptoms
- PMID: 21959689
- PMCID: PMC3271216
- DOI: 10.1007/s00464-011-1932-6
Long-term outcomes after transoral incisionless fundoplication in patients with GERD and LPR symptoms
Abstract
Background: A retrospective study evaluated safety, symptom resolution, patient satisfaction, and medication use 1-2 years after transoral incisionless fundoplication (TIF) in patients with gastroesophageal reflux disease (GERD) and/or laryngopharyngeal reflux (LPR) symptoms.
Methods: Thirty-four patients with a confirmed diagnosis of GERD symptoms that were inadequately controlled by antisecretory medications, and who where either dissatisfied with their current therapy or not willing to continue taking medication, underwent TIF using EsophyX at our community-based hospital. Follow-up assessments were completed in 28 patients.
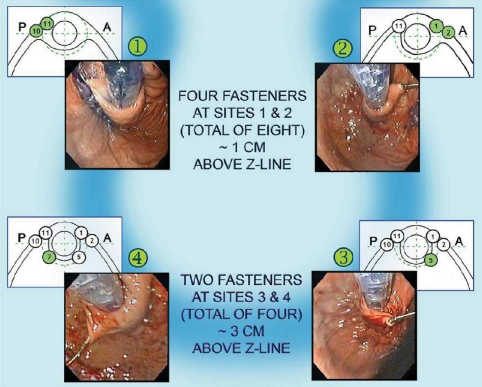
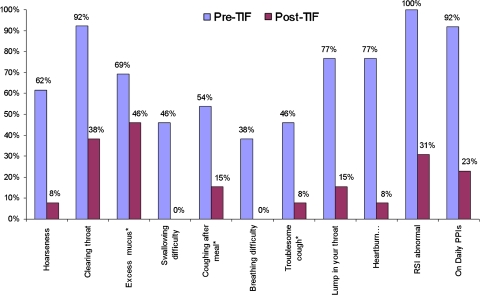
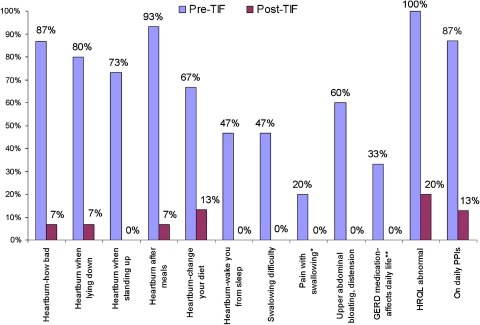
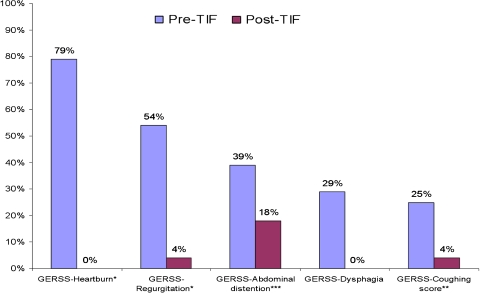
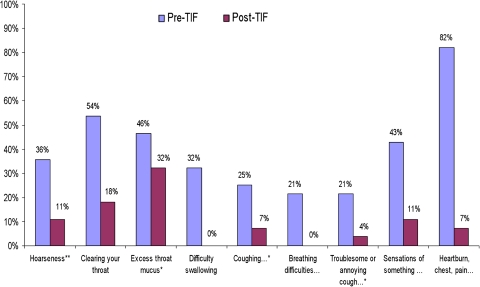
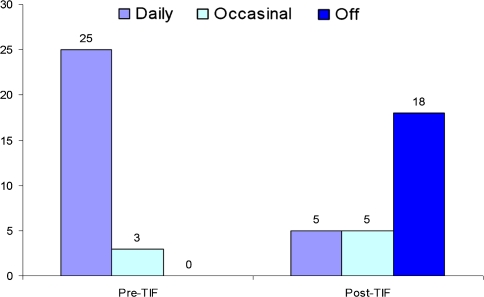
Results: Median age of the study group was 57 (range = 23-77) years, BMI was 25.7 (18.3-36.4) kg/m(2), and 50% were female. All patients had documented chronic GERD for a median 5 (1-20) years and refractory symptoms to proton pump inhibitors (PPIs). Hiatal hernia was present in 75% (21/28) of patients, and 21% (6/28) had erosive esophagitis (LA grade A or B). TIF was performed following a standardized TIF-2 protocol and resulted in reducing hiatal hernia and restoring the natural anatomy of the gastroesophageal (GE) junction (Hill grade I). There were no postoperative complications. At a median 14-months follow-up, 82% (23/28) of patients were off daily PPIs (64% completely off PPIs), and 68% (19/28) were satisfied with their current health condition compared to 4% before TIF. Median GERD Health-Related Quality of Life scores were significantly reduced to 4 (0-25) from 26 (0-45) before TIF (P < 0.001). Heartburn was eliminated in 65% (17/26) and improved by >50% in 86% (24/28) of patients. Regurgitation was eliminated in 80% (16/20) of patients. Atypical LPR symptoms such as hoarseness, coughing, and throat clearing were eliminated in 63% (17/27) of patients as measured by Reflux Symptom Index scores.
Conclusion: Our results in 28 patients confirm the safety and effectiveness of TIF, documenting symptomatic improvement of GERD and LPR symptoms and clinically significant discontinuation of daily PPIs in 82% of patients.
Figures
References
-
- Dallemagne B, Weerts JM, Jehaes C, Markiewicz S, Lombard R. Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc. 1991;1(3):138–143. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
