

Changes in PSA kinetics predict metastasis- free survival in men with PSA-recurrent prostate cancer treated with nonhormonal agents: combined analysis of 4 phase II trials
- PMID: 21960118
- PMCID: PMC3252493
- DOI: 10.1002/cncr.26437
Changes in PSA kinetics predict metastasis- free survival in men with PSA-recurrent prostate cancer treated with nonhormonal agents: combined analysis of 4 phase II trials
Abstract
Background: Several phase II trials in men with noncastrate PSA-recurrent prostate cancer have assessed the impact of novel nonhormonal agents on PSA kinetics. However, it is unknown whether changes in PSA kinetics influence metastasis-free survival (MFS).
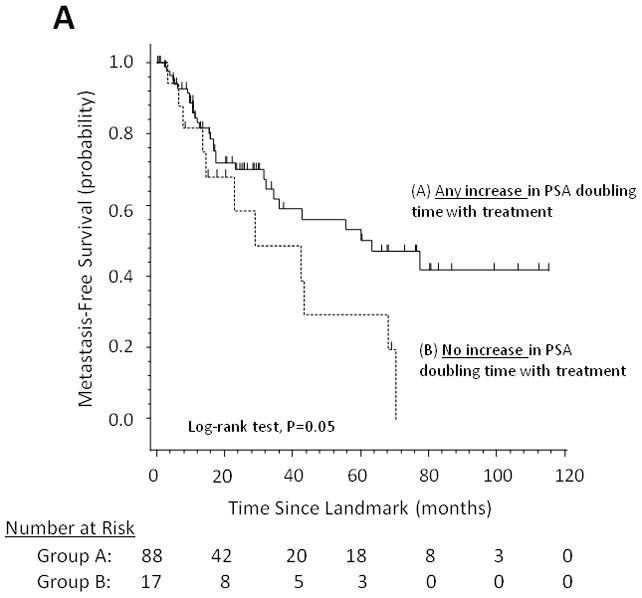
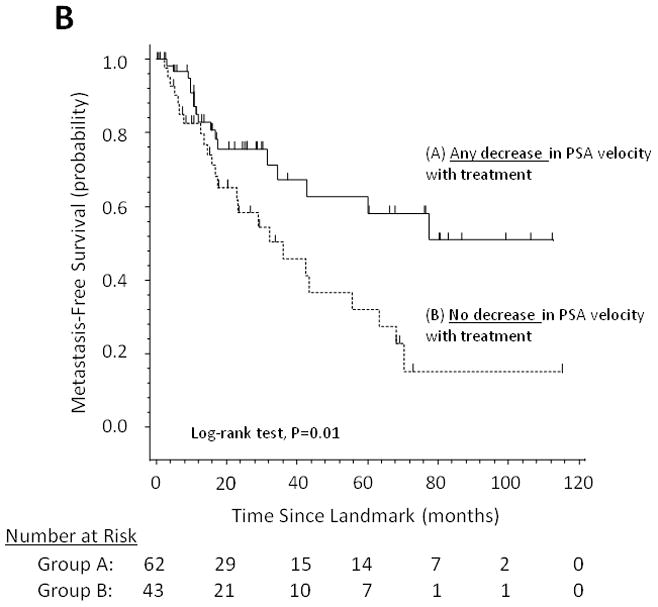
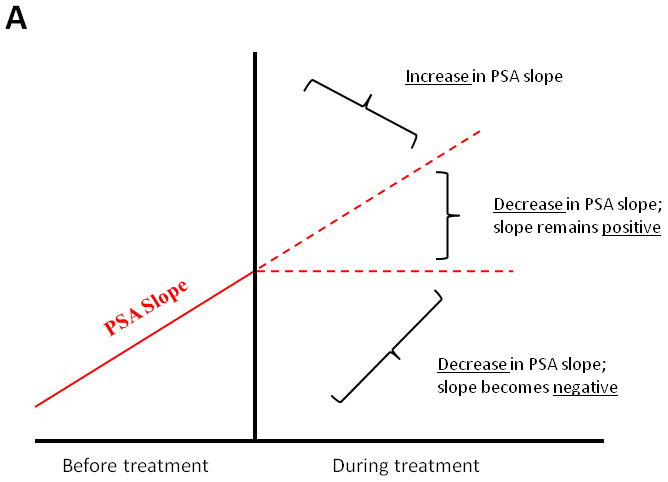
Methods: We performed a retrospective post hoc analysis of 146 men treated in 4 phase II trials examining the investigational agents marimastat (a matrix metalloproteinase inhibitor; n = 39), imatinib (a tyrosine kinase inhibitor; n = 25), ATN-224 (a copper/zinc-superoxide dismutase inhibitor; n = 22), and lenalidomide (an antiangiogenic/immunomodulatory drug; n = 60). We investigated factors influencing MFS, including within-subject changes in PSA kinetics (PSA slope, doubling time, and velocity) before and after treatment initiation.
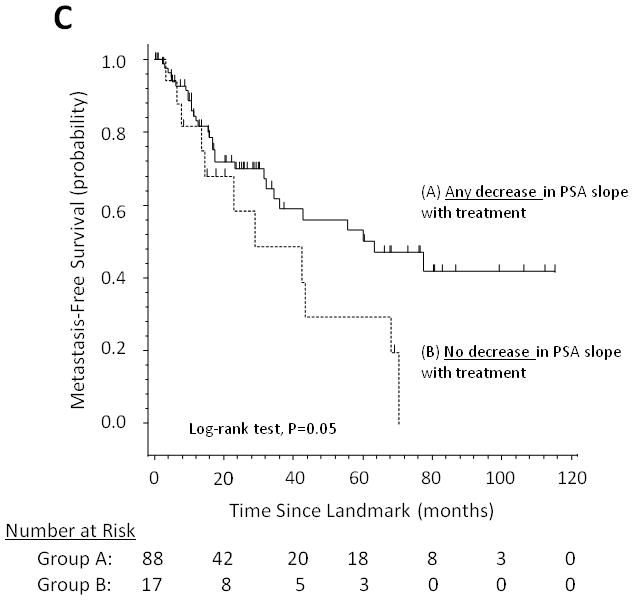
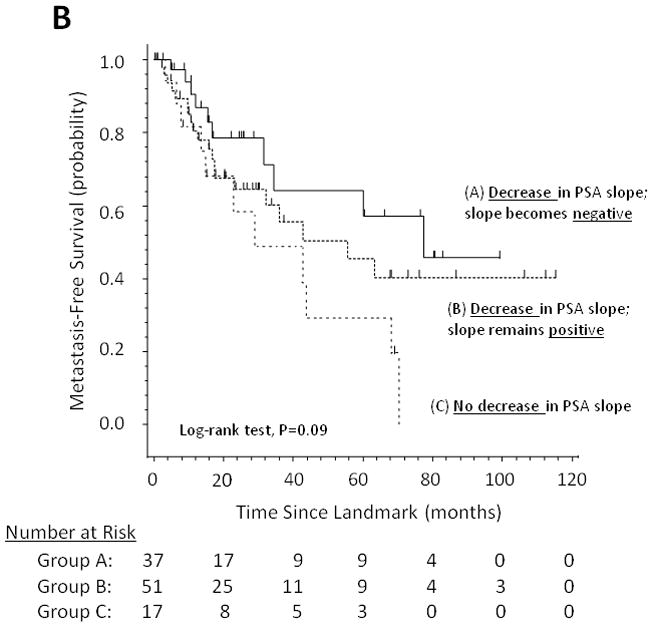
Results: After a median follow-up of 16.8 months, 70 patients (47.9%) developed metastases. In multivariable Cox regression models, factors that were independently predictive of MFS after adjusting for age and other clinical prognostic variables were baseline PSA doubling time (PSADT) (P = .05), baseline PSA slope (P = .01), on-study change in PSADT (P = .02), and on-study change in PSA slope (P = .03). In a landmark Kaplan-Meier analysis, median MFS was 63.5 months (95% confidence interval [CI], 34.6-not reached) and 28.9 months (95% CI, 13.5-68.0) for men with or without any decrease in PSA slope by 6 months after treatment, respectively.
Conclusions: This hypothesis generating analysis suggests that within-subject changes in PSADT and PSA slope after initiation of experimental therapy may correlate with MFS in men with biochemically recurrent prostate cancer. If validated in prospective trials, changes in PSA kinetics may represent a reasonable intermediate end point for screening new agents in these patients.
Conflict of interest statement
Figures
References
-
- Boccon-Gibod L, Djavan WB, Hammerer P, et al. Management of prostate-specific antigen relapse in prostate cancer: a European Consensus. Int J Clin Pract. 2004;58:382–390. - PubMed
-
- Sandler HM, Eisenberger MA. Assessing and treating patients with increasing prostate-specific antigen following radical prostatectomy. J Urol. 2007;178:S20–S24. - PubMed
-
- Antonarakis ES, Chen Y, Elsamanoudi SI, et al. Long-term overall survival and metastasis-free survival for men with prostate-specific antigen-recurrent prostate cancer after prostatectomy: analysis of the Center for Prostate Disease Research National Database. BJU Int. 2010 doi: 10.1111/j.1464-410X.2010.09878.x. (epub ahead of print) - DOI - PMC - PubMed
-
- Messing EM, Manola J, Yao J, et al. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol. 2006;7:472–479. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
