

Using quantitative CT perfusion for evaluation of delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage
- PMID: 21960495
- PMCID: PMC3237788
- DOI: 10.3174/ajnr.A2693
Using quantitative CT perfusion for evaluation of delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage
Abstract
Background and purpose: DCI is a serious complication following aneurysmal SAH leading to permanent neurologic deficits, infarction, and death. Our aim was to prospectively evaluate the diagnostic accuracy of CTP and to determine a quantitative threshold for DCI in aneurysmal SAH.
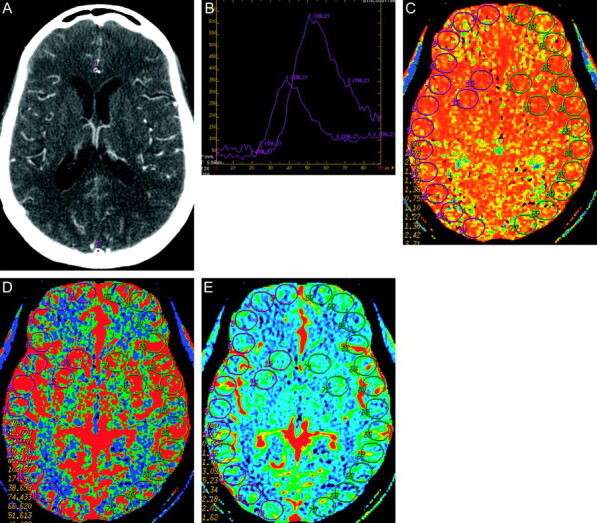
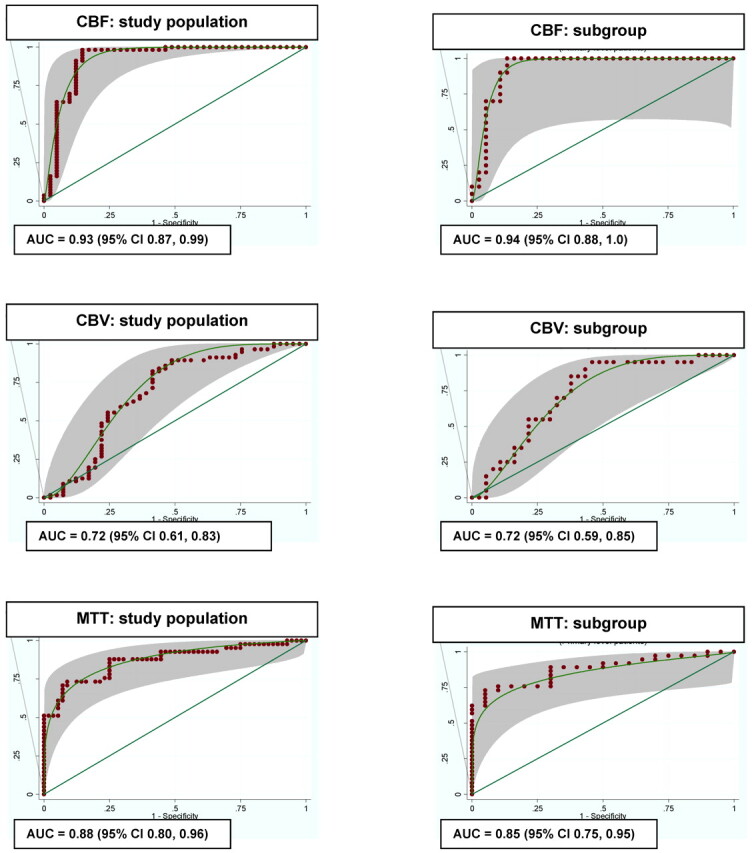
Materials and methods: Patients with SAH were prospectively enrolled in a protocol approved by the institutional review board. CTP was performed during the typical time period for DCI, between days 6 and 8 following SAH. Quantitative CBF, CBV, and MTT values were obtained by using standard region-of-interest placement sampling of gray matter. The reference standard for DCI is controversial and consisted of clinical and imaging criteria in this study. In a subanalysis of vasospasm, DSA was used as the reference standard. ROC curves determined the diagnostic accuracy by using AUC. Optimal threshold values were calculated by using the patient population utility method.
Results: Ninety-seven patients were included; 41% (40/97) had DCI. Overall diagnostic accuracy was 93% for CBF, 88% for MTT, and 72% for CBV. Optimal threshold values were 35 mL/100 g/min (90% sensitivity, 68% specificity) for CBF and 5.5 seconds (73% sensitivity, 79% specificity) for MTT. In the subanalysis (n = 57), 63% (36/57) had vasospasm. Overall diagnostic accuracy was 94% for CBF, 85% for MTT, and 72% for CBV. Optimal threshold values were 36.5 mL/100 g/min (95% sensitivity, 70% specificity) for CBF and 5.4 seconds (78% sensitivity, 70% specificity) for MTT.
Conclusions: CBF and MTT have the highest overall diagnostic accuracy. Threshold values of 35 mL/100 g/min for CBF and 5.5-second MTT are suggested for DCI on the basis of the patient population utility method. Absolute threshold values may not be generalizable due to differences in scanner equipment and postprocessing methods.
Figures
References
-
- Mayer SA, Kreiter KT, Copeland D, et al. Global and domain-specific cognitive impairment and outcome after subarachnoid hemorrhage. Neurology 2002;59:1750–58 - PubMed
-
- Hackett ML, Anderson CS. Health outcomes 1 year after subarachnoid hemorrhage: an international population-based study. Neurology 2000;55:658–62 - PubMed
-
- Solomon RA, Fink ME, Lennihan L. Early aneurysm surgery and prophylactic hypervolemic hypertensive therapy for the treatment of aneurysmal subarachnoid hemorrhage. Neurosurgery 1988;23:699–704 - PubMed
-
- Morgan MK, Jonker B, Finfer S, et al. Aggressive management of aneurysmal subarachnoid hemorrhage based on a papaverine angioplasty protocol. J Clin Neurosci 2000;7:305–08 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical