

Allergic fungal rhinosinusitis: a review
Abstract
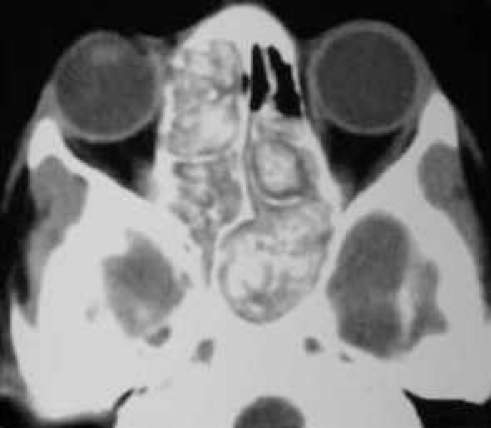
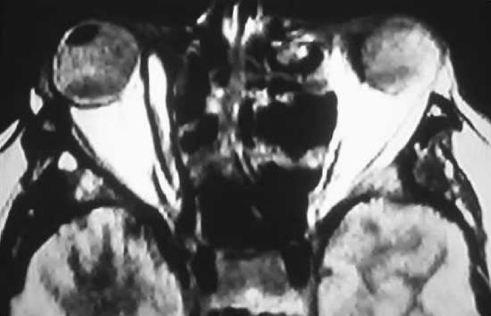
Background: Allergic fungal rhinosinusitis (AFRS) is a relatively new and incompletely understood clinical entity with characteristic clinical, radiographic, and histopathologic findings. AFRS is often misdiagnosed. Recognition and understanding of this unique disease will lead to efficient diagnosis and treatment of this curable process.
Methods: The following is a review, conducted via a PubMed English language search, of the current diagnosis, pathogenesis, and treatment of AFRS.
Results: AFRS is an immune-modulated disease entity. The Bent and Kuhn diagnostic criteria are the standard for diagnosis of this disease that occurs because of an incompletely understood allergic mechanism. Multimodality treatment relies heavily on surgical therapy along with corticosteroid use and immunotherapy.
Conclusions: AFRS is a unique disease process that differs from other forms of sinusitis and as such requires that physicians understand its diagnosis and management to provide care for patients with this condition.
Keywords: Allergic fungal sinusitis; Aspergillus; Bent and Kuhn; Bipolaris; allergic mucin; dematiaceous fungi; rhinosinusitis; sinusitis; type I and III hypersensitivity.
Figures
References
-
- Safirstein B. Allergic bronchopulmonary aspergillosis with obstruction of the upper respiratory tract. Chest. 1976;70:788–790. - PubMed
-
- Kuhn FA, Javer AR. Allergic fungal rhinosinusitis: our experience. Arch Otolaryngol Head Neck Surg. 1998;124(10):1179–1180. - PubMed
-
- Kuhn FA, Javer AR. Allergic fungal rhinosinusitis: perioperative management, prevention of recurrence, and role of steroids and antifungal agents. Otolaryngol Clin North Am. 2000;33(2):419–433. - PubMed
-
- Manning SC, Holman M. Further evidence for allergic pathophysiology in allergic fungal sinusitis. Laryngoscope. 1998;108(10):1485–1496. - PubMed
-
- Ryan MW, Marple BF. Allergic fungal rhinosinusitis: diagnosis and management. Curr Opin Otolaryngol Head Neck Surg. 2007;15(1):18–22. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources