

Right paraduodenal hernia in an adult patient: diagnostic approach and surgical management
- PMID: 21960952
- PMCID: PMC3180666
- DOI: 10.1159/000331033
Right paraduodenal hernia in an adult patient: diagnostic approach and surgical management
Abstract
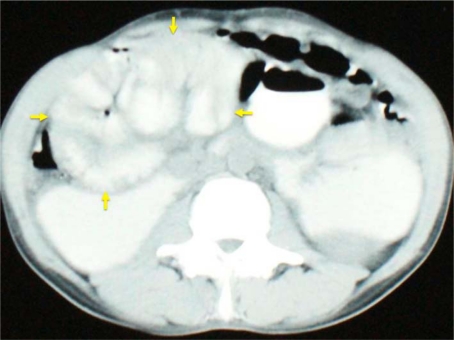
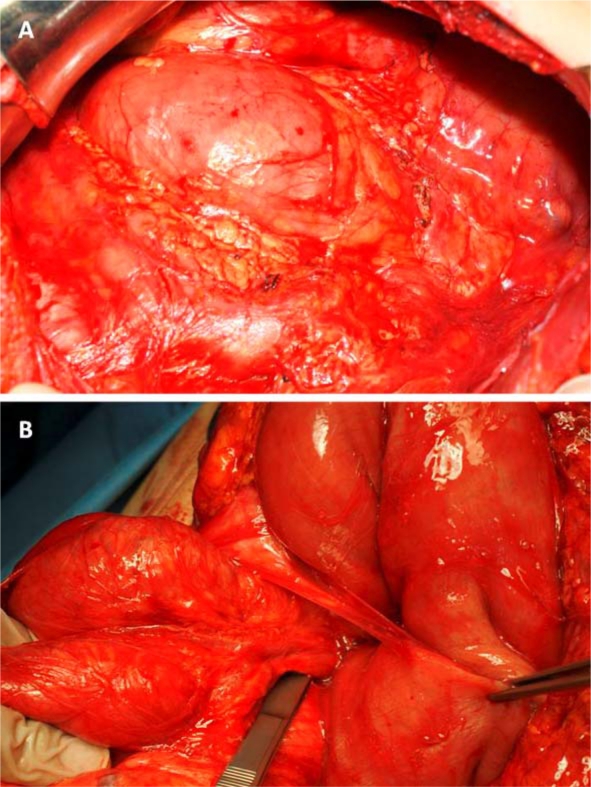
Paraduodenal hernia, a rare congenital anomaly which arises from an error of rotation of the midgut, is the most common type of intraabdominal hernia. There are two variants, right and left paraduodenal hernia, the right being less common. We report the case of a 41-year-old patient with a right paraduodenal hernia with a 6-month history of intermittent episodes of intestinal obstruction. Diagnosis was established by CT scan and upper gastrointestinal series with small bowel follow-through. In a planned laparotomy, herniation of the small bowel loops through the fossa of Waldeyer was found. Division of the lateral right attachments of the colon opened the hernia sac widely, replacing the pre- and postarterial segments of the intestine in the positions they would normally occupy at the end of the first stage of rotation during embryonic development. Six months after the surgery, after an uneventful recovery, the patient remains free of symptoms.
Keywords: Internal hernia; Intestinal obstruction; Paraduodenal hernia.
Figures

References
-
- Stern LE, Warner BW. Congenital internal abdominal hernias: incidence and management. In: Fitzgibbons RJ, Greenburg AG, editors. Nyhus and Condon's Hernia. 5th ed. Philadelphia: Lippincott Williams and Wilkins; 2002. pp. 453–465.
-
- Ghahremani GG. Internal abdominal hernias. Surg Clin North Am. 1984;64:393–406. - PubMed
-
- Hansmann GH, Morton SA. Intra-abdominal hernia: report of a case and review of the literature. Arch Surg. 1939;39:973–986.
-
- Khan MA, Lo AY, Vande Maele DM. Paraduodenal hernia. Am Surg. 1998;64:1218–1222. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
