

Radiation therapy for chloroma (granulocytic sarcoma)
- PMID: 21962486
- PMCID: PMC5045241
- DOI: 10.1016/j.ijrobp.2011.02.057
Radiation therapy for chloroma (granulocytic sarcoma)
Abstract
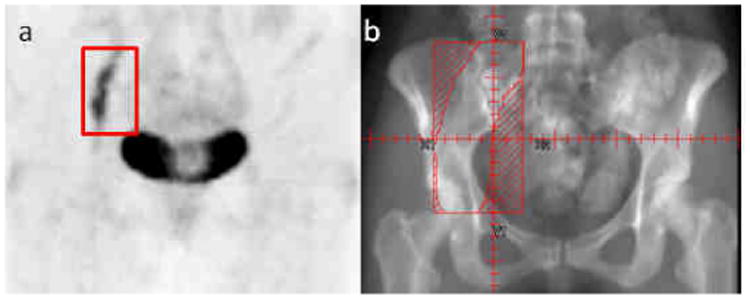
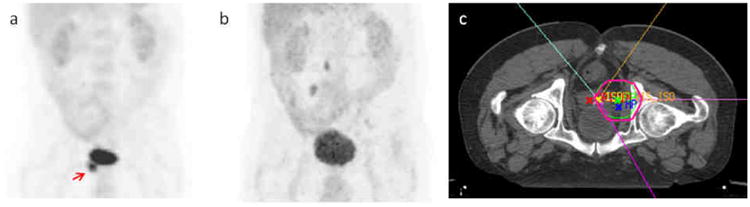
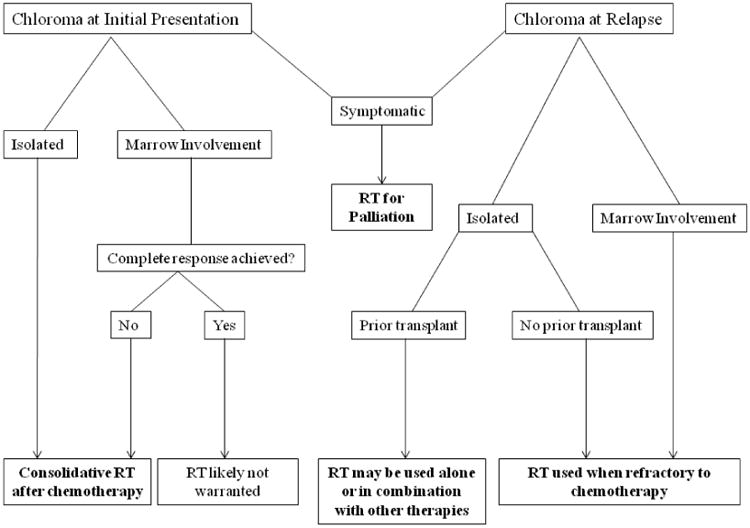
Objectives: Chloroma (granulocytic sarcoma) is a rare, extramedullary tumor of immature myeloid cells related to acute nonlymphocytic leukemia or myelodysplastic syndrome. Radiation therapy (RT) is often used in the treatment of chloromas; however, modern studies of RT are lacking. We reviewed our experience to analyze treatment response, disease control, and toxicity associated with RT to develop treatment algorithm recommendations for patients with chloroma.
Patients and methods: Thirty-eight patients who underwent treatment for chloromas at our institution between February 1990 and June 2010 were identified and their medical records were reviewed and analyzed.
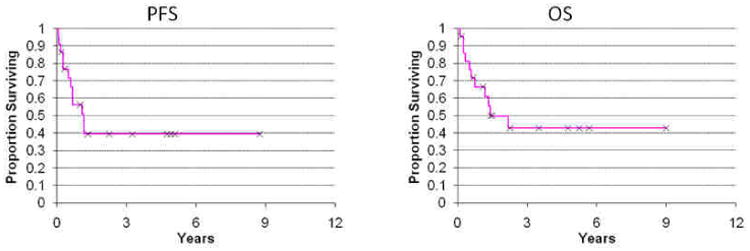
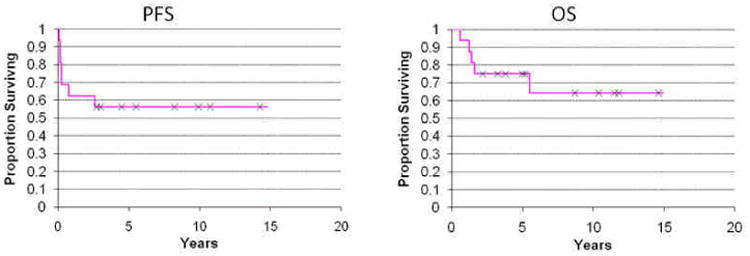
Results: The majority of patients that presented with chloroma at the time of initial leukemia diagnosis (78%) have not received RT because it regressed after initial chemotherapy. Yet most patients that relapsed or remained with chloroma after chemotherapy are in the RT cohort (90%). Thirty-three courses of RT were administered to 22 patients. Radiation subsite breakdown was: 39% head and neck, 24% extremity, 9% spine, 9% brain, 6% genitourinary, 6% breast, 3% pelvis, and 3% genitourinary. Median dose was 20 (6-36) Gy. Kaplan-Meier estimates of progression-free survival and overall survival in the RT cohort were 39% and 43%, respectively, at 5 years. At a median follow-up of 11 months since RT, only 1 patient developed progressive disease at the irradiated site and 4 patients developed chloromas at other sites. RT was well tolerated without significant acute or late effects and provided symptom relief in 95% of cases.
Conclusions: The majority of patients with chloromas were referred for RT when there was extramedullary progression, marrow relapse, or rapid symptom relief required. RT resulted in excellent local disease control and palliation of symptoms without significant toxicity. We recommend irradiating chloromas to at least 20 Gy, and propose 24 Gy in 12 fractions as an appropriate regimen.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Notification: The authors have no actual or potential conflicts of interest.
Figures
References
-
- Burns A. Observations of surgical Anatomy in Head and Neck. Edinburg: Thomas Royce; 1811.
-
- King A. A case of Chloroma. Monthly J Med. 1853;17:97.
-
- Reardon G, Moloney WC. Chloroma and related myeloblastic neoplasms. Arch Intern Med. 1961;108:864–871. - PubMed
-
- Rappaport H. Tumors of the hematopoietic system, in Atlas of Tumor Pathology, Section III, Fascicle 8. Armed Forces Institute of Pathology; Washington D.C.: 1967.
-
- Neiman RS, Barcos M, Berard C, et al. Granulocytic sarcoma: a clinicopathologic study of 61 biopsied cases. Cancer. 1981;48:1426–1437. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
