

Therapeutic response to vasoconstrictors in hepatorenal syndrome parallels increase in mean arterial pressure: a pooled analysis of clinical trials
- PMID: 21962618
- PMCID: PMC3251915
- DOI: 10.1053/j.ajkd.2011.07.017
Therapeutic response to vasoconstrictors in hepatorenal syndrome parallels increase in mean arterial pressure: a pooled analysis of clinical trials
Abstract
Background: Vasoconstrictor therapy has been advocated as treatment for hepatorenal syndrome (HRS). Our aim was to explore across all tested vasoconstrictors whether achievement of a substantial increase in arterial blood pressure is associated with recovery of kidney function in HRS.
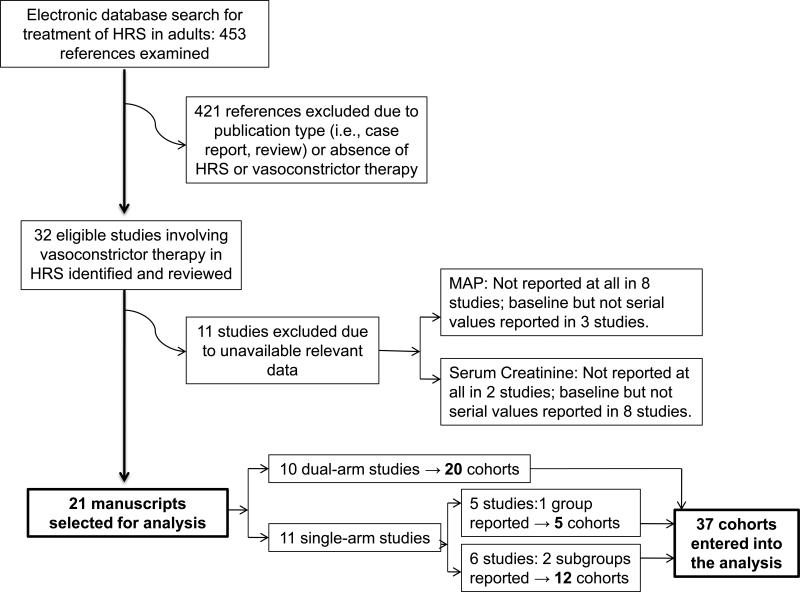
Study design: Pooled analysis of published studies identified by electronic database search.
Setting & population: Data pooled across 501 participants in 21 studies.
Selection criteria for studies: Human studies evaluating the efficacy of a vasoconstrictor administered for 72 hours or longer in adults with HRS type 1 or 2.
Intervention: Vasoconstrictor therapy.
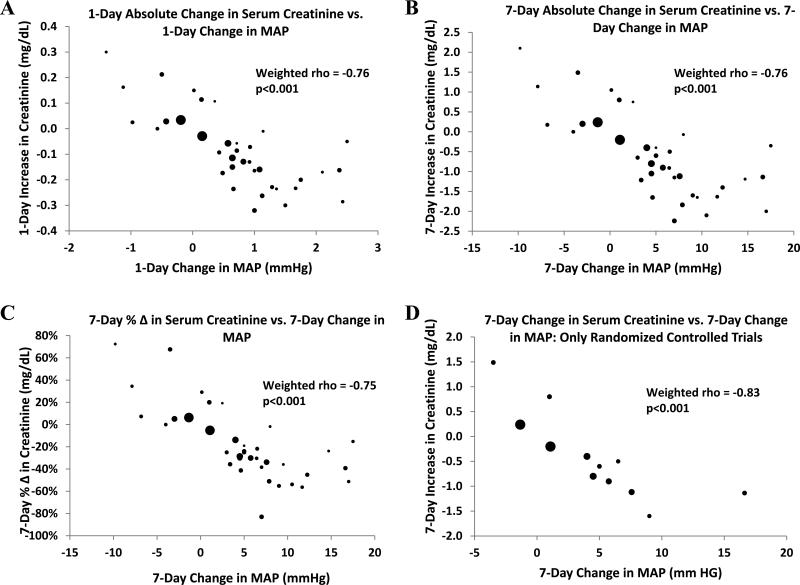
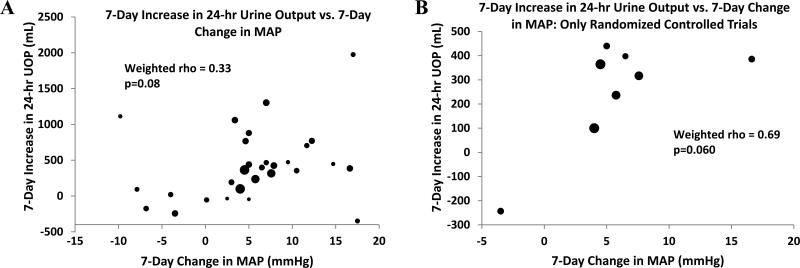
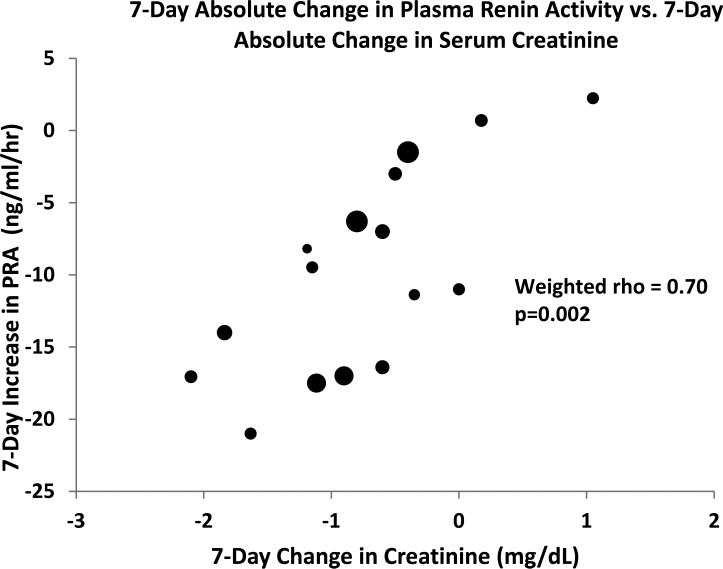
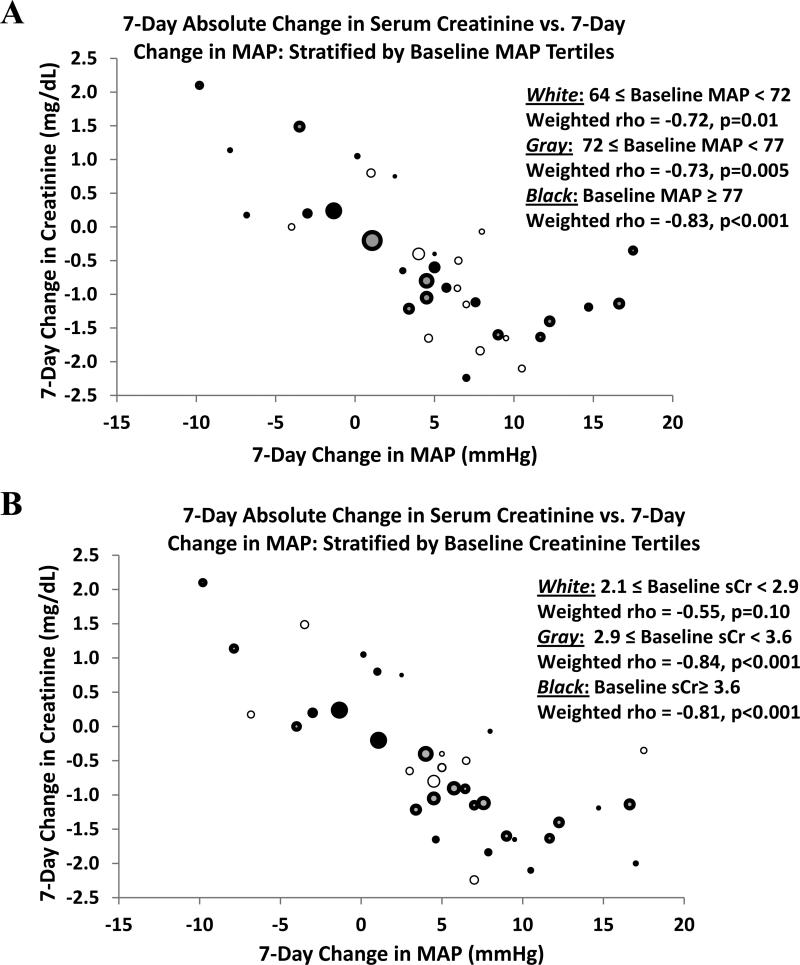
Outcomes & measurements: Cohorts' mean arterial pressure (MAP), serum creatinine level, urinary output, and plasma renin activity (PRA) at baseline and subsequent times during treatment. Linear regression models were constructed to estimate mean daily changes in MAP, serum creatinine level, urinary output, and PRA for each study subgroup. Correlations were used to assess for association between variables.
Results: An increase in MAP is associated strongly with a decrease in serum creatinine level, but is not associated with an increase in urinary output. Associations were stronger when analyses were restricted to randomized clinical trials and were not limited to cohorts with either lower baseline MAP or lower baseline serum creatinine level. Most studies tested terlipressin as vasoconstrictor, whereas fewer studies tested ornipressin, midodrine, octreotide, or norepinephrine. Excluding cohorts of participants treated with terlipressin or ornipressin did not eliminate the association. Furthermore, a decrease in PRA correlated with improvement in kidney function.
Limitations: Studies were not originally designed to test our question. We lacked access to individual patient data.
Conclusions: An increase in MAP during vasoconstrictor therapy in patients with HRS is associated with improvement in kidney function across the spectrum of drugs tested to date. These results support consideration for a goal-directed approach to the treatment of HRS.
Copyright © 2011 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Epstein M, et al. Renal failure in the patient with cirrhosis. The role of active vasoconstriction. Am J Med. 1970;49:175–185. - PubMed
-
- Gines P, Schrier RW. Renal failure in cirrhosis. N Engl J Med. 2009;361:1279–1290. - PubMed
-
- Ring-Larsen H. Renal blood flow in cirrhosis: relation to systemic and portal haemodynamics and liver function. Scand J Clin Lab Invest. 1977;37:635–642. - PubMed
-
- Arroyo V, Terra C, Gines P. Advances in the pathogenesis and treatment of type-1 and type-2 hepatorenal syndrome. J Hepatol. 2007;46:935–946. - PubMed
-
- Moreau R, Lebrec D. Acute kidney injury: new concepts. Hepatorenal syndrome: the role of vasopressors. Nephron Physiol. 2008;109:p73–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
