

Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial
- PMID: 21963002
- PMCID: PMC3208163
- DOI: 10.1016/S0140-6736(11)60937-9
Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial
Abstract
Background: Back pain remains a challenge for primary care internationally. One model that has not been tested is stratification of the management according to the patient's prognosis (low, medium, or high risk). We compared the clinical effectiveness and cost-effectiveness of stratified primary care (intervention) with non-stratified current best practice (control).
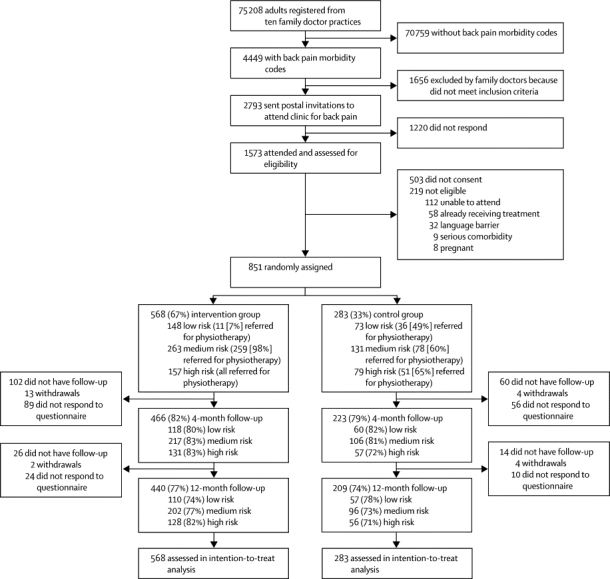
Methods: 1573 adults (aged ≥18 years) with back pain (with or without radiculopathy) consultations at ten general practices in England responded to invitations to attend an assessment clinic. Eligible participants were randomly assigned by use of computer-generated stratified blocks with a 2:1 ratio to intervention or control group. Primary outcome was the effect of treatment on the Roland Morris Disability Questionnaire (RMDQ) score at 12 months. In the economic evaluation, we focused on estimating incremental quality-adjusted life years (QALYs) and health-care costs related to back pain. Analysis was by intention to treat. This study is registered, number ISRCTN37113406.
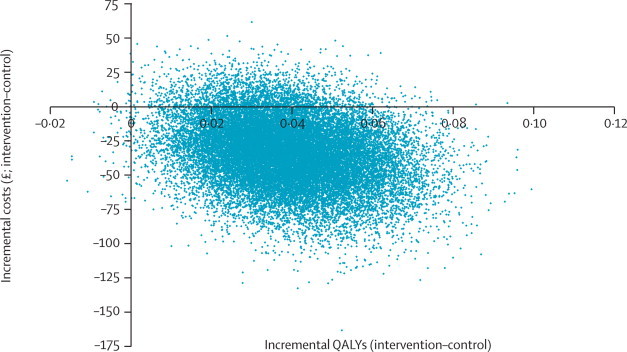
Findings: 851 patients were assigned to the intervention (n=568) and control groups (n=283). Overall, adjusted mean changes in RMDQ scores were significantly higher in the intervention group than in the control group at 4 months (4·7 [SD 5·9] vs 3·0 [5·9], between-group difference 1·81 [95% CI 1·06-2·57]) and at 12 months (4·3 [6·4] vs 3·3 [6·2], 1·06 [0·25-1·86]), equating to effect sizes of 0·32 (0·19-0·45) and 0·19 (0·04-0·33), respectively. At 12 months, stratified care was associated with a mean increase in generic health benefit (0·039 additional QALYs) and cost savings (£240·01 vs £274·40) compared with the control group.
Interpretation: The results show that a stratified approach, by use of prognostic screening with matched pathways, will have important implications for the future management of back pain in primary care.
Funding: Arthritis Research UK.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Management of low back pain in primary care: a new approach.Lancet. 2011 Oct 29;378(9802):1530-2. doi: 10.1016/S0140-6736(11)61033-7. Epub 2011 Sep 28. Lancet. 2011. PMID: 21963003 No abstract available.
-
[Stratified management of patients with lumbar backache in primary care].Praxis (Bern 1994). 2012 Feb 1;101(3):199-200. doi: 10.1024/1661-8157/a000850. Praxis (Bern 1994). 2012. PMID: 22294307 German. No abstract available.
-
Targeted physiotherapy treatment for low back pain based on clinical risk can improve clinical and economic outcomes when compared with current best practice.J Physiother. 2012;58(1):57. doi: 10.1016/S1836-9553(12)70073-5. J Physiother. 2012. PMID: 22341383
-
ACP Journal Club. Risk-stratified primary care management of low back pain reduced disability.Ann Intern Med. 2012 Feb 21;156(4):JC2-07. doi: 10.7326/0003-4819-156-4-201202210-02007. Ann Intern Med. 2012. PMID: 22351733 No abstract available.
References
-
- WHO The burden of musculoskeletal conditions at the start of the new millennium. World Health Organ Tech Rep Ser. 2003;919:1–218. - PubMed
-
- Costa-Black KM, Loisel P, Anema JR, Pransky G. Back pain and work. Best Pract Res Clin Rheumatol. 2010;24:227–240. - PubMed
-
- Dunn KM, Croft PR. Classification of low back pain in primary care: using “bothersomeness” to identify the most severe patients. Spine. 2005;130:1887–1892. - PubMed
-
- McGrail MP, Jr, Lohman WH, Gorman R. Disability prevention principles in the primary care office. Am Fam Phys. 2001;63:679–684. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
