

National Cancer Institute-National Heart, Lung and Blood Institute/pediatric Blood and Marrow Transplant Consortium First International Consensus Conference on late effects after pediatric hematopoietic cell transplantation: long-term organ damage and dysfunction
- PMID: 21963877
- PMCID: PMC3215762
- DOI: 10.1016/j.bbmt.2011.09.013
National Cancer Institute-National Heart, Lung and Blood Institute/pediatric Blood and Marrow Transplant Consortium First International Consensus Conference on late effects after pediatric hematopoietic cell transplantation: long-term organ damage and dysfunction
Abstract
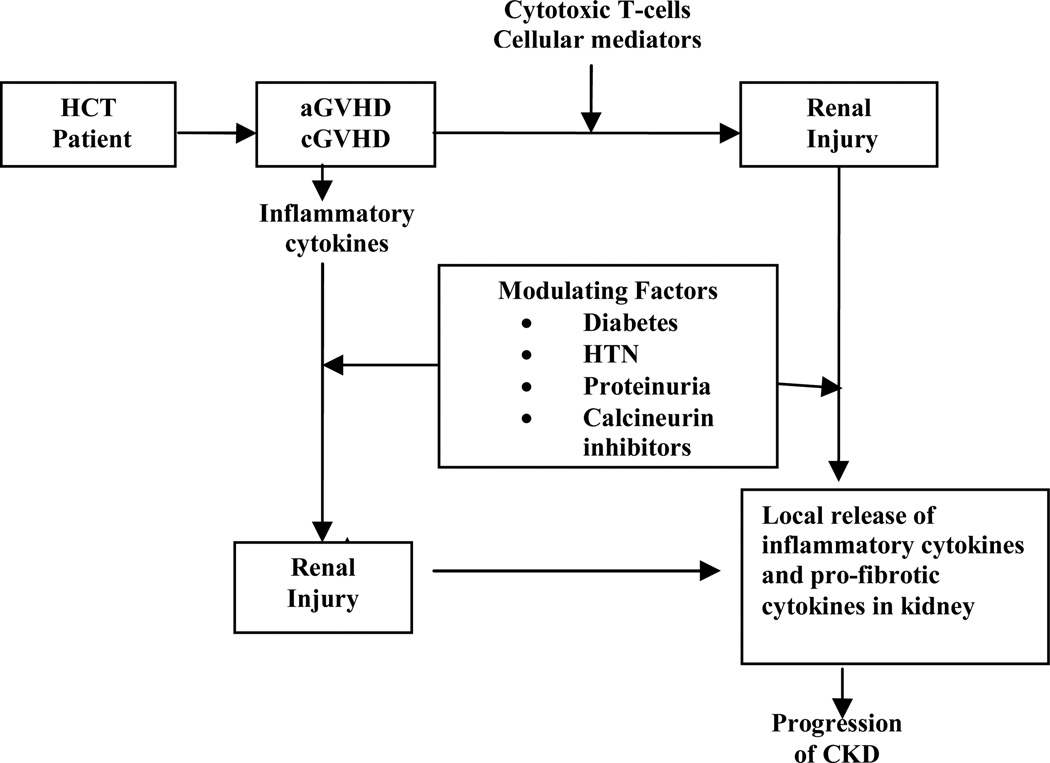
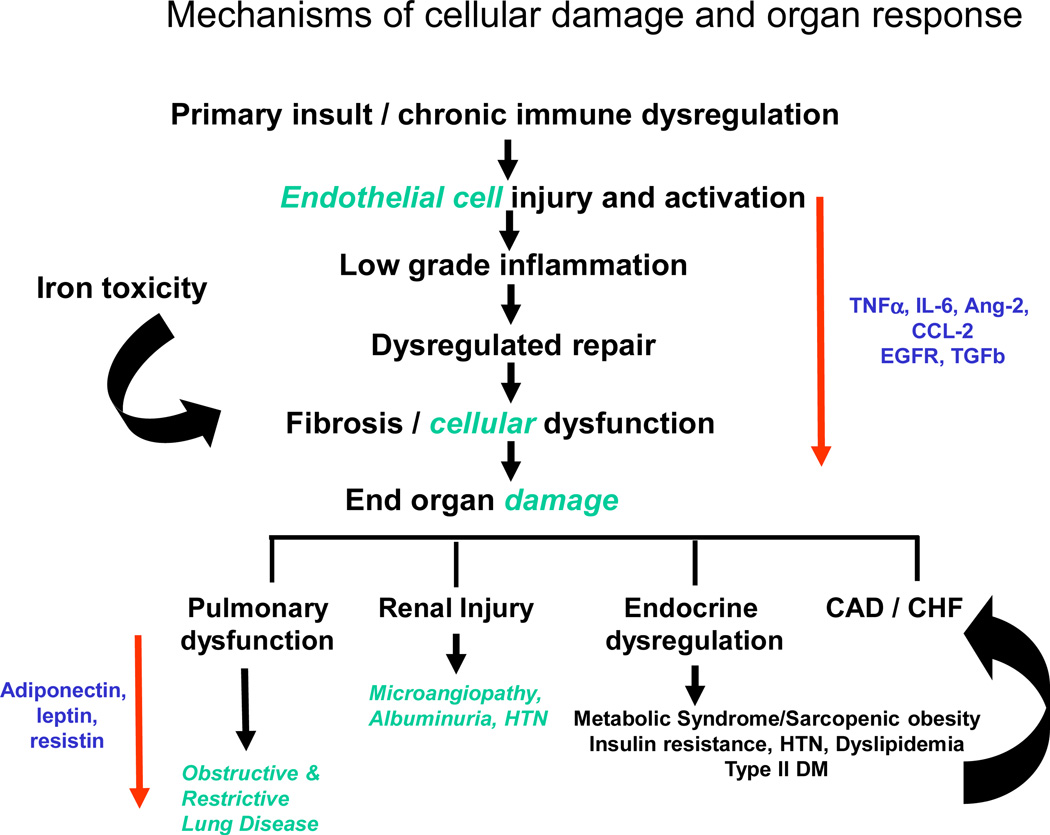
Long-term complications after hematopoietic cell transplantation (HCT) have been studied in detail. Although virtually every organ system can be adversely affected after HCT, the underlying pathophysiology of these late effects remain incompletely understood. This article describes our current understanding of the pathophysiology of late effects involving the gastrointestinal, renal, cardiac, and pulmonary systems, and discusses post-HCT metabolic syndrome studies. Underlying diseases, pretransplantation exposures, transplantation conditioning regimens, graft-versus-host disease, and other treatments contribute to these problems. Because organ systems are interdependent, long-term complications with similar pathophysiologic mechanisms often involve multiple organ systems. Current data suggest that post-HCT organ complications result from cellular damage that leads to a cascade of complex events. The interplay between inflammatory processes and dysregulated cellular repair likely contributes to end-organ fibrosis and dysfunction. Although many long-term problems cannot be prevented, appropriate monitoring can enable detection and organ-preserving medical management at earlier stages. Current management strategies are aimed at minimizing symptoms and optimizing function. There remain significant gaps in our knowledge of the pathophysiology of therapy-related organ toxicities disease after HCT. These gaps can be addressed by closely examining disease biology and identifying those patients at greatest risk for adverse outcomes. In addition, strategies are needed for targeted disease prevention and health promotion efforts for individuals deemed at high risk because of their genetic makeup or specific exposure profile.
Copyright © 2011 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Hentze MW, Muckenthaler MU, Andrews NC. Balancing acts: molecular control of mammalian iron metabolism. Cell. 2004;117:285–297. - PubMed
-
- Majhail NS, Lazarus HM, Burns LJ. A prospective study of iron overload management in allogeneic hematopoietic cell transplantation survivors. Biol Blood Marrow Transplant. 2010;16:832–837. - PubMed
-
- Strasser SI, Kowdley KV, Sale GE, McDonald GB. Iron overload in bone marrow transplant recipients. Bone Marrow Transplant. 1998;22:167–173. - PubMed
-
- Mariotti E, Angelucci E, Agostini A, Baronciani D, Sgarbi E, Lucarelli G. Evaluation of cardiac status in iron-loaded thalassaemia patients following bone marrow transplantation: improvement in cardiac function during reduction in body iron burden. British Journal of Haematology. 1998;103:916–921. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
