

Variability in usual care mechanical ventilation for pediatric acute lung injury: the potential benefit of a lung protective computer protocol
- PMID: 21965099
- PMCID: PMC3589567
- DOI: 10.1007/s00134-011-2367-1
Variability in usual care mechanical ventilation for pediatric acute lung injury: the potential benefit of a lung protective computer protocol
Abstract
Purpose: Although pediatric intensivists claim to embrace lung protective ventilation for acute lung injury (ALI), ventilator management is variable. We describe ventilator changes clinicians made for children with hypoxemic respiratory failure, and evaluate the potential acceptability of a pediatric ventilation protocol.
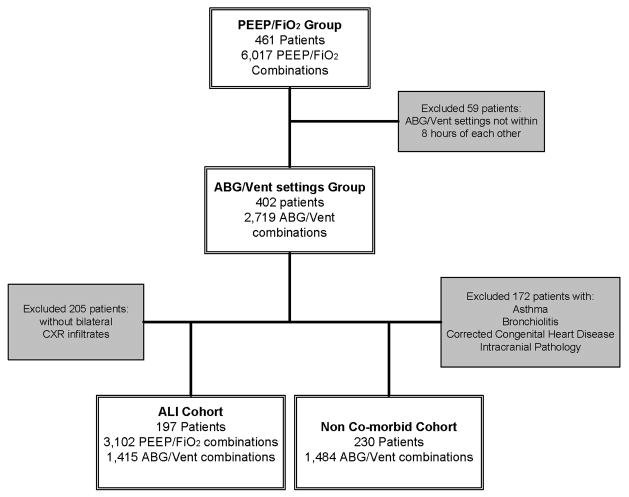
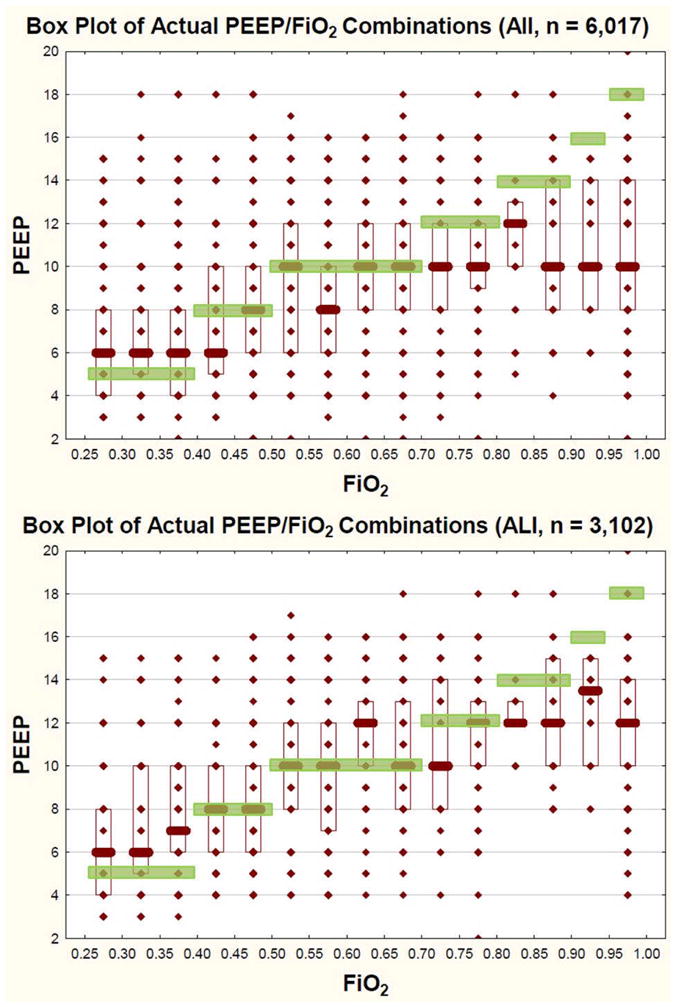
Methods: This was a retrospective cohort study performed in a tertiary care pediatric intensive care unit (PICU). The study period was from January 2000 to July 2007. We included mechanically ventilated children with PaO(2)/FiO(2) (P/F) ratio less than 300. We assessed variability in ventilator management by evaluating actual changes to ventilator settings after an arterial blood gas (ABG). We evaluated the potential acceptability of a pediatric mechanical ventilation protocol we adapted from National Institutes of Health/National Heart, Lung, and Blood Institute (NIH/NHLBI) Acute Respiratory Distress Syndrome (ARDS) Network protocols by comparing actual practice changes in ventilator settings to changes that would have been recommended by the protocol.
Results: A total of 2,719 ABGs from 402 patients were associated with 6,017 ventilator settings. Clinicians infrequently decreased FiO(2), even when the PaO(2) was high (>68 mmHg). The protocol would have recommended more positive end expiratory pressure (PEEP) than was used in actual practice 42% of the time in the mid PaO(2) range (55-68 mmHg) and 67% of the time in the low PaO(2) range (<55 mmHg). Clinicians often made no change to either peak inspiratory pressure (PIP) or ventilator rate (VR) when the protocol would have recommended a change, even when the pH was greater than 7.45 with PIP at least 35 cmH(2)O.
Conclusions: There may be lost opportunities to minimize potentially injurious ventilator settings for children with ALI. A reproducible pediatric mechanical ventilation protocol could prompt clinicians to make ventilator changes that are consistent with lung protective ventilation.
Figures
References
-
- Santschi M, Jouvet P, Leclerc F, Gauvin F, Newth CJ, Carroll C, Flori H, Tasker RC, Rimensberger P, Randolph A PALIVE Investigators, PALISI Network, ESPNIC. Acute lung injury in children: therapeutic practice and feasibility of international clinical trials. Pediatr Crit Care Med. 2010;11:681–689. - PubMed
-
- ARDSnet. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301–1308. - PubMed
-
- Putensen C, Theuerkauf N, Zinserling J, Wrigge H, Pelosi P. Meta-analysis: ventilation strategies and outcomes of the acute respiratory distress syndrome and acute lung injury. Ann Intern Med. 2009;151:566–576. - PubMed
-
- Villar J, Kacmarek RM, Perez-Mendez L, Aguirre-Jaime A. A high positive end-expiratory pressure, low tidal volume ventilatory strategy improves outcome in persistent acute respiratory distress syndrome: a randomized, controlled trial. Critical Care Medicine. 2006;34:1311–1318. - PubMed
-
- Umoh NJ, Fan E, Mendez-Tellez PA, Sevransky JE, Dennison CR, Shanholtz C, Pronovost PJ, Needham DM, Umoh NJ, Fan E, Mendez-Tellez PA, Sevransky JE, Dennison CR, Shanholtz C, Pronovost PJ, Needham DM. Patient and intensive care unit organizational factors associated with low tidal volume ventilation in acute lung injury. Critical Care Medicine. 2008;36:1463–1468. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
